Download to read offline






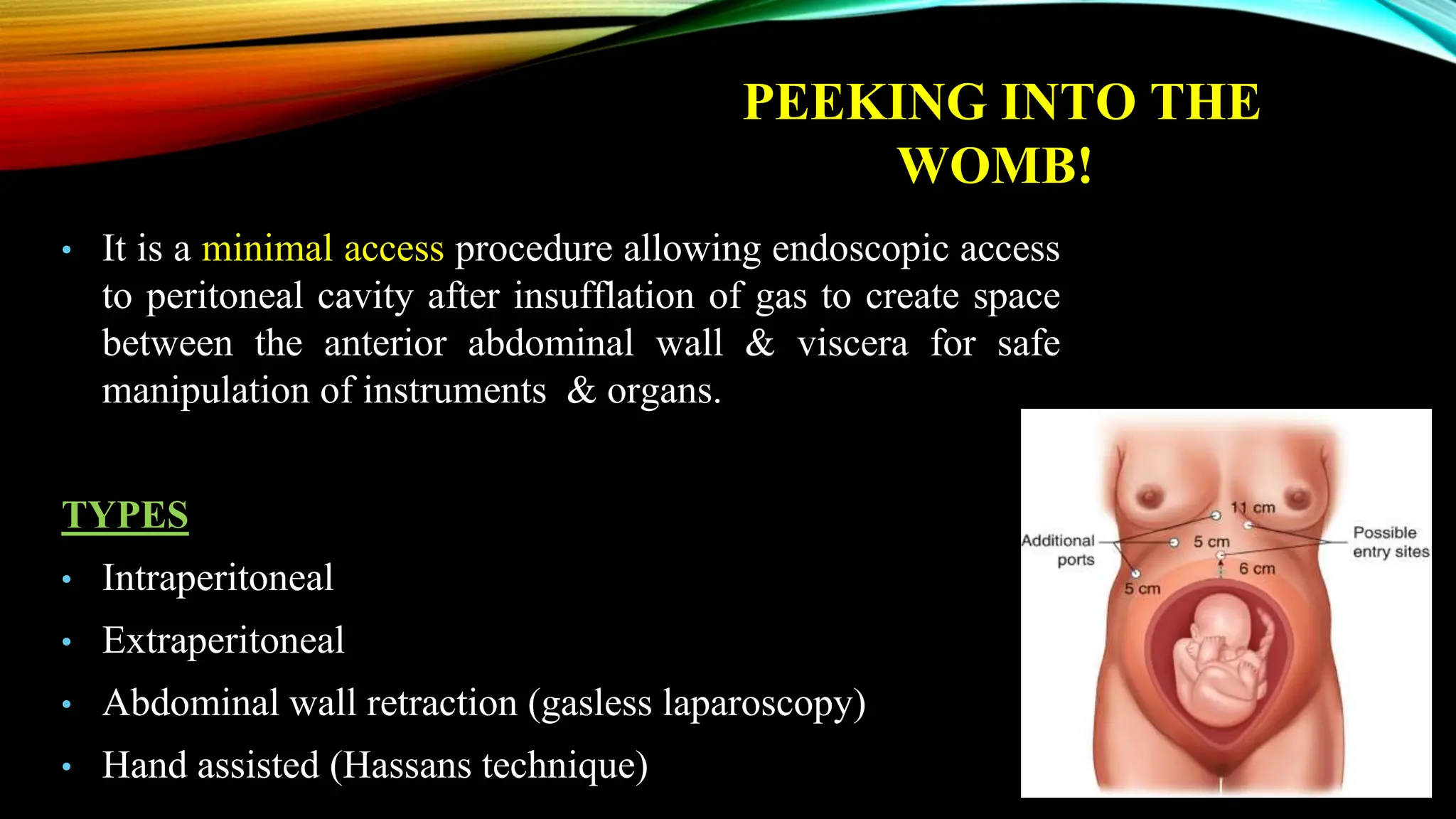



































The document discusses the use of laparoscopy in pregnancy, detailing its history, types, indications, advantages over open surgery, and safety considerations. It highlights guidelines for implementation, complications, risks associated with procedures, and presents case studies illustrating practical applications. Laparoscopy is emphasized as a minimal access approach that can be effectively performed during any trimester, with specific precautions to ensure maternal and fetal safety.



































































