Diabetic Maculopathy1 Gos2
•Download as PPT, PDF•
7 likes•981 views

This document discusses diabetic maculopathy and macular edema. It covers the causes of vision loss, classifications of diabetic retinopathy, types of macular edema, clinically significant macular edema (CSME), treatment options including laser photocoagulation, a clinical study on treating CSME with focal and grid laser, and conclusions about the importance of early recognition and treatment.
![How is the vision lost? ,[object Object],[object Object],[object Object]](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Diabetic Maculopathy1 Gos2
Similar to Diabetic Maculopathy1 Gos2 (20)
More from Dr. Anand Sudhalkar
More from Dr. Anand Sudhalkar (20)
Diabetic Maculopathy1 Gos2
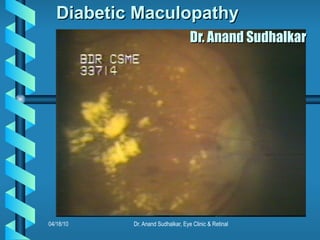
- 1. Diabetic Maculopathy Dr. Anand Sudhalkar
- 11. FFA taken 4 years Apart F.A.Z. enlargement
- 12. Principles of Management : Laser delivery Slit-Lamp Magnification Enlarged & Steady View
- 14. Pre-laser FFA microaneurisms
- 19. Sub-classification Focal and Diffuse Pre-treatment Visual Acuity
- 20. 04/18/10 Assessment of Results
- 25. Message : ETDRS REPORT 19 Recommends photocoagulation before the foveal vision loss occurs In clinically significant diabetic macular oedema
- 26. Diabetes and Cataract Exacerbation after Cataract Surgery
- 28. Thank You all for patient hearing
Editor's Notes
- Blindness due to diabetic retinopathy affects the adult population20 to 64 yr. age and is as common a complication of diabetes as end stage renal disease and nontraumatic lower limb amputations. Long standing hyperglycaemia causes loss of endothelial pericytes and thickening of basement membrane of capillaries resulting in breaking down of endothelial barrier and narrowing of lumen, causing retinal oedema and capillary closures.
- Vision can be diminished due to macular oedema, ischaemia or exudates Vitreous haemorrhage, or TRD. Vitreous haemorrhage occurs in PDR and causes sudden drop in vision.Tractional retinal detachment is the end stage complication along with neovascularization.
- Two broad classifications NPDR-previous BDR and PDR. NPDR is further subclassified from treatment point of view into mild moderate and severe depending upon occurrences of dot haemorrhages, microeneurysms and exudates. The severe form needs special mention due to it's importance in decision making for PRP and guidelines laid are Blot haemo. in 4 qdrs., venous beading in 2 qdrs. and IRMA in 1 qdr. If two or more of these are present, 45% can go into PDR in a years time.
- We will be discussing macular oedema as a cause for visual loss. There are two basic types but clinically some overlapping does occur. The focal type is due to a leaking microaneurysm, the exudate is a high molecular weight lipoprotein clinically constituting hard exudates and spreading around the culprit microaneurysm in a circinate pattern. The diffuse oedema is due to capillary leakage oozing out low molecular weight watery fluid creating cystoid spaces. Usually the condition is bilateral and associated with systemic conditions like H.T., renal failure, anemia and hypoprotenemia.
- When would this condition cause visual disturbances? It is when the foveal region is threatened. Early identification of this situation is done by slit-lamp biomicroscopy using fundus contact or non contact lenses. The central 500mu circle of foveal avascular area is scrutinised for the retinal thickening. Even if the centre of fovea is not involved, the danger to visual acuity exists if the pathology is touching the boundary. A large area of retinal oedema even a disc diameter away from centre of macula is clinically significant from treatment point of view.
- How common is the condition ? Is the trouble of considering this worth it's while? The answer lies here. Ten percent of all diabetics will have some kind of retinopathy. Of those who have retinopathy, 40% will have CSME i.e 2.5% of all diabetics need some laser treatment. If you consider only BDR cases 3% need attention for CSME. The prevalence increases with advancing retinopathy to 38% for PPDR and 71% in PDR group. 5% of maturity onset insulin dependent diabetics have retinopathy at the time diagnoses and not uncommon to have ophthalmologist diagnose it from fundus examination for the first time. The prevalence of the disease is directly proportionate with duration of hyperglycaemia.
- Diabetis control and complications trial was a prospective and randomised clinical trial designed to study the connection between glycacaemic control and retinal, renal and neurologic complications. Control of hyperglycaemia is shown to help in delaying the onset and slowing the progression of retinopathy in type 1 IDDM. On the other hand in cases of mild to moderate NPDR in NIDDM who were put under strict control later on, showed worsening of retinopathy. Hence in clinically significant cases photocoagulation should not be delayed in waiting for blood sugar to be normal. Control of HT, renal failure, anaemia, hypoprotemia are helpful adjuvants to photocoagulation. Laser photocoagulation is the treatment for macular oedema and has been supported by many clinical trials out of which early treatment diabetic retinopathy study needs special mention. It is one of the best scientifically conducted multicentric prospective trials in the field of medicine as a whole and not only ophthalmology.
- It was aimed to judge the efficacy of laser treatment for macular oedema, to decide about optimal timing to initiate PRP in cases of severe NPDR and to evaluate the role of aspirin in management of diabetic retinopathy.
- Fluorescein angiography helped in differentiating focal and diffuse oedema and identified the culprit microaneurysms in focal oedema group. This made laser treatment with slit-lamp delivery and Mainster lens more precise. The cases were followed up at regular intervals and repeat FFA & additional laser treatment give as required.
- FFA though not essential for diagnosis of CSME, is useful in locating the leaking MA in focal edema, understanding capillary drop-outs and dilatations in diffuse edema, mapping out FAZ and diagnosis of macular ischemia. It can also help in locating IRMA and early NV.
- Progressive enlargement of FAZ is seen with advancing retinopathy. This can greatly worsen the prognosis and laser will not help.
- Steady and variable magnification, choice of spot size, safeguarding foveola, pricision of laser delivery are possible only with good slitlamp delivery system. Choice for various contact lenses lies with the surgeon, I prefer mainster lens for it’s wide field. This keeps the disc, macula and arcades in view and prevents foveal burns. The picture is inverted but with practice it does not bother us.
- The focal macular oedema is treated by coagulating the culprit microaneurysm identified by FFA or one present in the centre of circinate exudate. Excessive burns should be avoided in other areas.
- Slide on left shows exudates close to fovea and FFA picture on right shows MA
- On left are the fresh laser burns and on right the photograph after three months.
- Grid pattern photocoagulation for defuse macular edema. 500 mu from centre of foveola and lateral margin of disc are spared.
- We reviewed our cases of BDR with CSME to analyse the results of focal and grid laser photocoagulation and to compare the visual gain in early and late treated cases
- Total of 90 eyes from 66 patients were reviewed. Excluding the other possible ocular causes of vision loss, associated systemic conditions like Hypertension and impaired cardiac and renal status which may contribute to the loss of visual acuity.
- Out of 68 eyes with focal oedema, 53 had visual acuity > or = 6/36. 15 had vision <6/36 at the time of treatment. Out of the diffuse oedema group, all presented with vision < 6/36.
- The results were analysed as per the improvement in vision on Snellen's chart by more than one or two lines. In the focal oedema group the improvement was noted in 61 of 68 eyes by one line and 32 of 68 eyes by two lines. Out of 22 eyes in the diffuse oedema group treated with grid laser, improvement was noted 14 eyes for more than one line and 5 eyes gained more than two lines.
- The cases which presented with initial visual acuity better than or - 6/36, had better gain in post laser vision than those which presented with vision < 6/36.
- Early treatment for CSME has shown better results as the foveal function is not yet compromised.
- Inability to judge CSME early, leads a physician and sometimes an ophthalmologist to avoid reference for laser even in symptomatic patients. They advise better control of diabetes and delay laser treatment. Some ophthalmologists are known to start antioxidents, asperin and even steroids and worsen the prognosis by avoiding early laser treatment. Non avaibility of laser machines is one of the causes.
- This means advising photocoagulation even with 6/6 vision if clinically the fundus picture shows CSME
- Missing diabetic retinopathy before cataract surgery can ruin the results of good phaco as there is sudden worsening of retinopathy within a month post-op.
- Regular followup is necessary even after successful treatment for CSME to recognise the signs of early PDR. Early initiation of PRP is advocated by ETDRS if the other eye has PDR, if cataract surgery is due, if patient is pregnant, if follow up is irregular. Once vitreous haemorrhage occrs, laser treatment becomes difficult.