
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Diabetic macular edema
Similar to Diabetic macular edema (20)
More from abhishek ghelani
More from abhishek ghelani (20)
Recently uploaded
Recently uploaded (20)
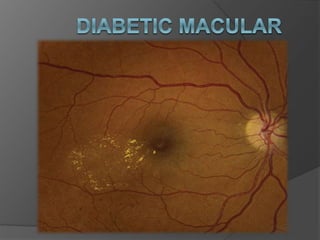
Diabetic macular edema
- 2. INTRODUCTION • Diabetic retinopathy is one of the leading cause of blindness. • Duration of diabetes is a major risk factor associated with the development of diabetic retinopathy. After 5 years, approximately 25% of Type 1 patients will have retinopathy. After 10 years, almost 60% have retinopathy, and after 15 years, 80% have retinopathy. • In type 2 DM, it depends on • Duration of disease • Accompnying hypertension • And smoking
- 3. CLASSIFICATION OF DIABETIC RETINOPATHY 1. Non –proliferative diabetic retinopathy (NPDR) • Mild • Moderate to severe 2. Proliferative diabetic retinopathy(PDR) 3. Maculopathy • Diffuse or focal • CSME • Ischemic maculopathy
- 5. DEFINITION OF DME • It is the retinal thickening caused by intraretinal leakage of fluid primarily in inner and outer plexiform layer due to increased capillary permiability • It can be present with any level of DR • RISK FACTORS • Duration of Diabetes Mellitus (DM) • Poor control of DM with chronically elevated hemoglobin A1c (HbA1c) • Hypertension • Hyperlipidemia
- 7. PATHGENESIS Normal retinal capillaries are non fenestrated and has blood retinal barrier that does not allow leakage of fluid Retina also does not have lymphatic system, so leaked fluid is accumulated and cause edema Chronic hyperglycemia-related accumulation of advanced glycated end products (AGEs) causes disruption of the blood retinal barrier (BRB) and an altered vitreo-retinal interface. Altered BRB leads to interstitial fluid accumulation within the retina and, in some cases, cyst formation, particularly in the perifoveal retina.
- 8. Histopathological examination of the eyes with diabetic retinopathy shows • loss of intramural pericytes, • thickening of the basement membrane and • progressive closure of the retinal capillaries. • The initial loss of pericytes leads to dilatation of the vessels (microaneurysm, the first sign seen on fuduscopy) and breakdown of BRB In addition there is increased aggregation of platelets, causing capillary non perfusion • Extensive closure of capillaries leads to ischaemia that leads to opening of shunt vessels “IRMA” and neovascularisation by elaborating VEGF
- 9. CSME It is defined as edema or hard exudates within 500 micrometer of the foveal centre or Edema of more than one disc area in extent, any part of which is within 1 DD of the foveal centre
- 10. DIFFRENTIAL DIAGNOSIS • ARMD (Exudative) • BRVO • CRVO • Hypertension maculopathy • Irvine-Gass syndrome • Uveitis • Epinephrine use in aphakia • Hypotonic retinopathy • Ruptured microaneurysm • Radiation retinopathy • Subfoveal choroidal neovascularization
- 11. DIAGNOSTIC PROCEDURES • Optical coherence tomography (OCT) OCT shows three basic structural changes: 1. retinal swelling, 2. cystoid macular edema, and 3. subretinal fluid.
- 12. OCT is a more sensitive method for objective evaluation of vitreo-macular traction and for measurement of macular thickness. OCT is more sensitive at detecting retinal thickening than is biomicroscopy. Experienced examiners generally cannot detect retinal thickening until retinal thickness is ≥ 300 µm. OCT is not required to establish the diagnosis according to current guidelines but its an additional modality that allow identification and evaluation of macular pathology And it also allow presice and reproducible way to monitor macular edema
- 13. FFA Fluorescein Angiography (FA) FA is performed to identify leaking microaneurysms or capillaries and areas of retinal ischemia. Leakage on the angiogram is not synonymous with retinal edema. Focal CSME is characterized by focal leakage from microaneurysms or capillaries whereas diffuse DME is diagnosed when poorly demarcated areas of leakage are present on the FA.
- 15. MANAGEMENT • DIET • LIFESTYLE CHANGES PREVENTION • People with Type 1 diabetes should have annual screenings for diabetic retinopathy beginning 5 years after the onset of their disease, • whereas those with Type 2 diabetes should have a prompt examination at the time of diagnosis and at least yearly examinations thereafter. • Women who develop gestational diabetes do not require an eye examination during pregnancy • However, patients with diabetes who become pregnant should be examined early in the course of the pregnancy.
- 16. TREATMENT MEDICAL CARE Control of diabetis Life style modification Diet OCCULAR TREATMENT LASER Anti VEGF Steroids
- 17. LASER Photocoagulation (Focal or Grid) GOALS • To reduce progression • It reduces the risk of moderate visual loss from diabetic macular edema by 50%, from 24% to 12% 3 years after initiation of treatment. TIMING • It is most effective when initiated before visual acuity is lost from diabetic macular edema • LASER treatment of DME should precede PRP by at least 2-6 weeks because PRP before this has been known to worsen DME. • PRP should not be delayed in very severe NPDR or high risk PDR. Multiple sessions over many months are frequently necessary for resolution of DME
- 18. Side effects and complications of focal LASER • Paracentral scotomata • Transient increased edema/decreased vision • Choroidal neovascularization • Subretinal fibrosis • Inadvertent foveolar burns
- 19. Normal or Minimal NPDR • The patient with a normal retinal examination or minimal NPDR (i.e., with rare microaneurysms) should be re-examined annually, because within 1 year 5% to 10% of patients without retinopathy will develop diabetic retinopathy. • Laser, color fundus photography, and FA are not necessarily indicated.
- 20. Mild to Moderate NPDR without Macular Edema • Patients should be re-examined within 6 to 12 months, because disease progression is common. • Laser and FA are not indicated for this group of patients. • Color fundus photography and OCT imaging of the macula may occasionally be helpful to establish a baseline for future comparison and for patient education. • Patients with macular edema that is not clinically significant should be re-examined within 3 to 4 months, because they are at significant risk of developing CSME.
- 21. Mild to Moderate NPDR with CSME • Fluorescein angiography prior to laser surgery for CSME is often helpful for identifying treatable lesions. • Fluorescein angiography is less relevant when there are circinate lipid exudates and the leaking lesions are clearly detected within the lipid ring. • Fluorescein angiography is also useful for detecting capillary dropout and pathologic enlargement of the foveal avascular zone, a feature that may be useful when planning treatment The traditional treatment for CSME has been laser. However, current data from multiple well-designed studies demonstrate that intravitreal anti-VEGF agents provide a more effective treatment for center-involved CSME than monotherapy with laser.
- 22. Anti-VEGF Therapy • At the present time, anti-VEGF therapy is the initial treatment choice for center-involving macular edema, with possible subsequent or deferred focal laser treatment. • The Ranibizumab for Edema of the mAcula in Diabetes (READ- 2) study involved 126 patients randomized to either anti-VEGF therapy (in this case ranibizumab alone), laser alone, or focal/grid laser combined with anti-VEGF therapy. • The group that received anti-VEGF therapy alone or with laser treatment did better than the group treated with laser alone. • The Diabetic Retinopathy Clinical Research Network (DRCR.net) also showed that anti-VEGF with either prompt or deferred laser photocoagulation was better than either laser alone or laser combined with triamcinolone acetonide.
- 23. • Bevacizumab or Laser Treatment (BOLT) study also showed favorable outcomes for bevacizumab use over macular laser treatment in eyes with ci-CSME. • The DME and VEGF Trap-Eye: Investigation of Clinical Impact (DA VINCI) study demonstrated better outcomes using aflibercept over laser treatment for ci-CSME. • Most recently, the DRCR.net protocol T demonstrated that anti-VEGF therapy using bevacizumab, ranibizumab, or aflibercept is an effective treatment for center-involving CSME. However, at worse levels of initial visual acuity (20/50 or worse), aflibercept was more effective at improving visual acuity than the other anti-VEGF agents tested.
- 24. • With the advent of anti-VEGF therapy for macular edema, many retina specialists prefer to use a modified ETDRS(Early Treatment Diabetic Retinopathy Study) treatment approach. • This includes a less intense laser treatment, greater spacing, directly targeting microaneurysms, and avoiding foveal vasculature within at least 500 µm of the center of the macula.
- 25. Severe NPDR and Non-High-Risk PDR • Severe NPDR and non-high-risk PDR are discussed together because the ETDRS data showed that they have a similar clinical course and subsequent recommendations for treatment are similar. • the ETDRS suggested that panretinal photocoagulation should not be recommended for eyes with mild or moderate NPDR, provided that follow-up could be maintained. When retinopathy is more severe, panretinal photocoagulation should be considered
- 26. • Careful follow-up at 3 to 4 months is important: • if the patient will not or cannot be followed closely or if there are associated medical conditions such as impending cataract surgery or pregnancy, early laser panretinal photocoagulation may be warranted • Currently, the role of anti-VEGF therapy in the management of severe NPDR and non-high-risk PDR is under investigation.
- 27. High-Risk PDR • New vessels within one disc diameter of the optic nerve head that are larger than one-quarter to one-third disc area in size • New vessels elsewhere that are at least one-half disc area in size • Vitreous or preretinal hemorrhage • Very recently, the DRCR.net study protocol S has demonstrated that alternative use of anti-VEGF agents (ranibizumab was used in this protocol), may be an alternative to PRP. • However, many feel that PRP remains the first choice for management of PDR. The anti-VEGF alternative could be considered for patients who can follow-up regularly. • Further studies are required to determine the long-term implications of using anti-VEGF agents alone.
- 28. Additional panretinal photocoagulation, anti-VEGF therapy, or vitrectomy surgery may be necessary for the following situations: • Failure of the neovascularization to regress • Increasing neovascularization of the retina or iris • New vitreous hemorrhage • New areas of neovascularization