Downloaded 15 times
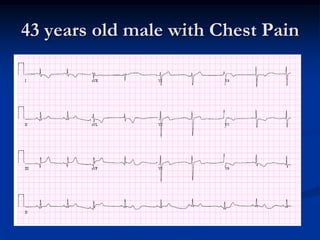

1) A 43-year-old male presented with chest pain and was diagnosed with an acute inferior STEMI while in normal sinus rhythm. His medical history included atherosclerosis. 2) Atherosclerosis is caused by plaque buildup in arteries and accounts for over 70% of cardiovascular deaths in the US. Elevated LDL cholesterol increases the risk of atherosclerosis and heart disease. 3) Therapeutic lifestyle changes like diet and exercise can modestly lower LDL cholesterol by about 5% on average but response varies between individuals. High fat, low carb diets may improve glycemic control in diabetes without worsening lipids.






























































































