Downloaded 62 times










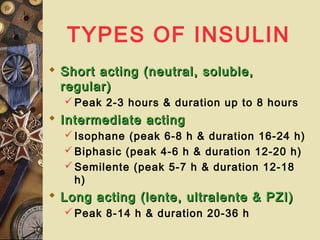
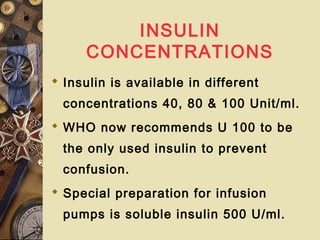
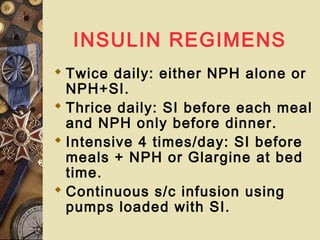
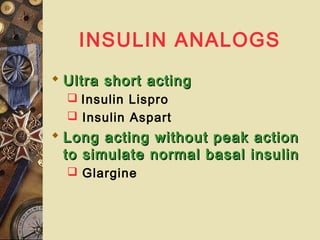




This document discusses childhood diabetes mellitus. It defines diabetes as a metabolic disorder characterized by chronic hyperglycemia. Type 1 diabetes accounts for over 90% of childhood cases and is an autoimmune disease triggered by environmental factors in genetically susceptible individuals. Proper treatment involves education, insulin therapy tailored to the individual, diet and exercise, and regular monitoring to prevent complications and achieve metabolic control goals. Advances allow more precise glucose monitoring and individualized insulin regimens.























































































