Downloaded 297 times
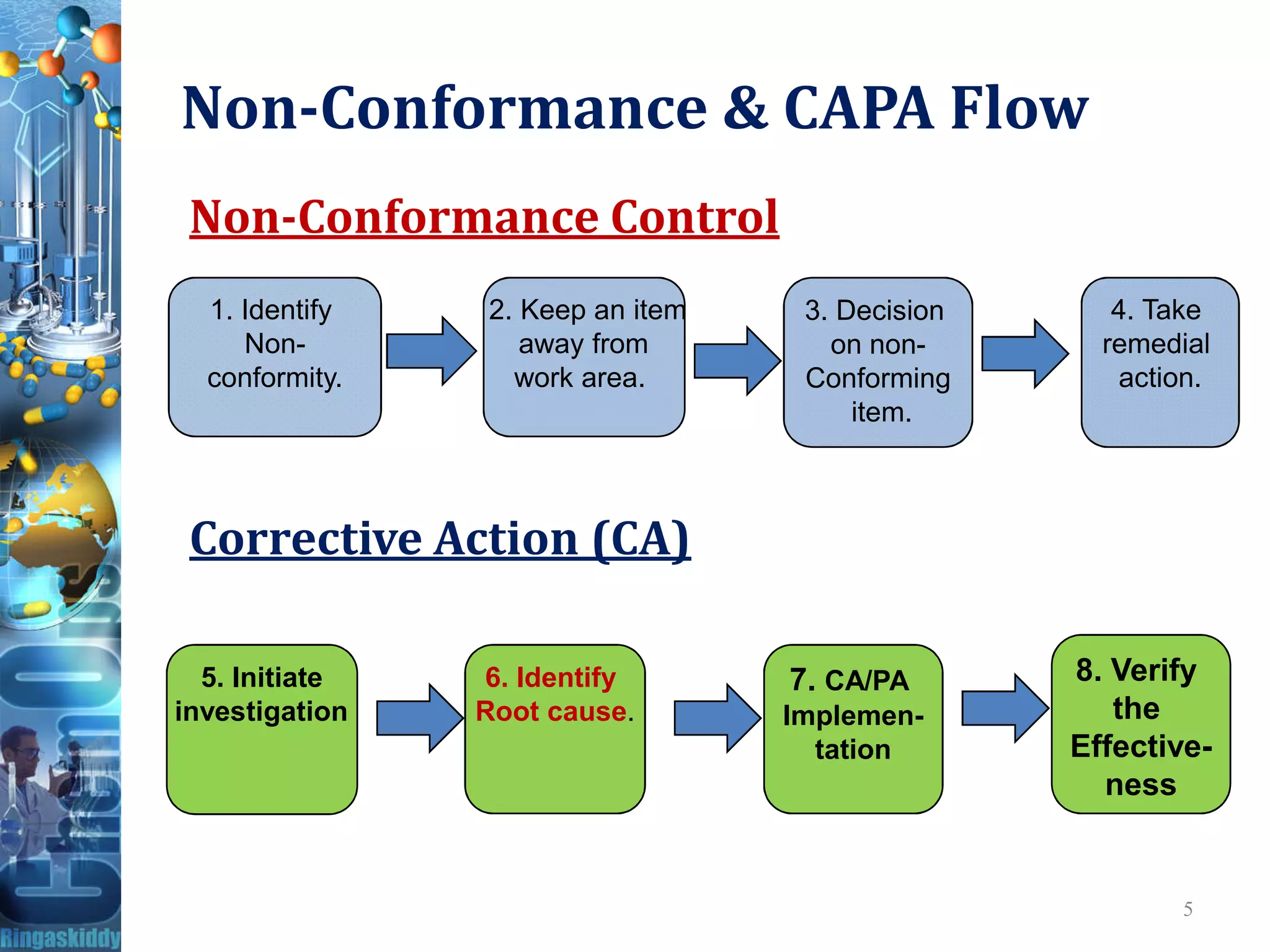
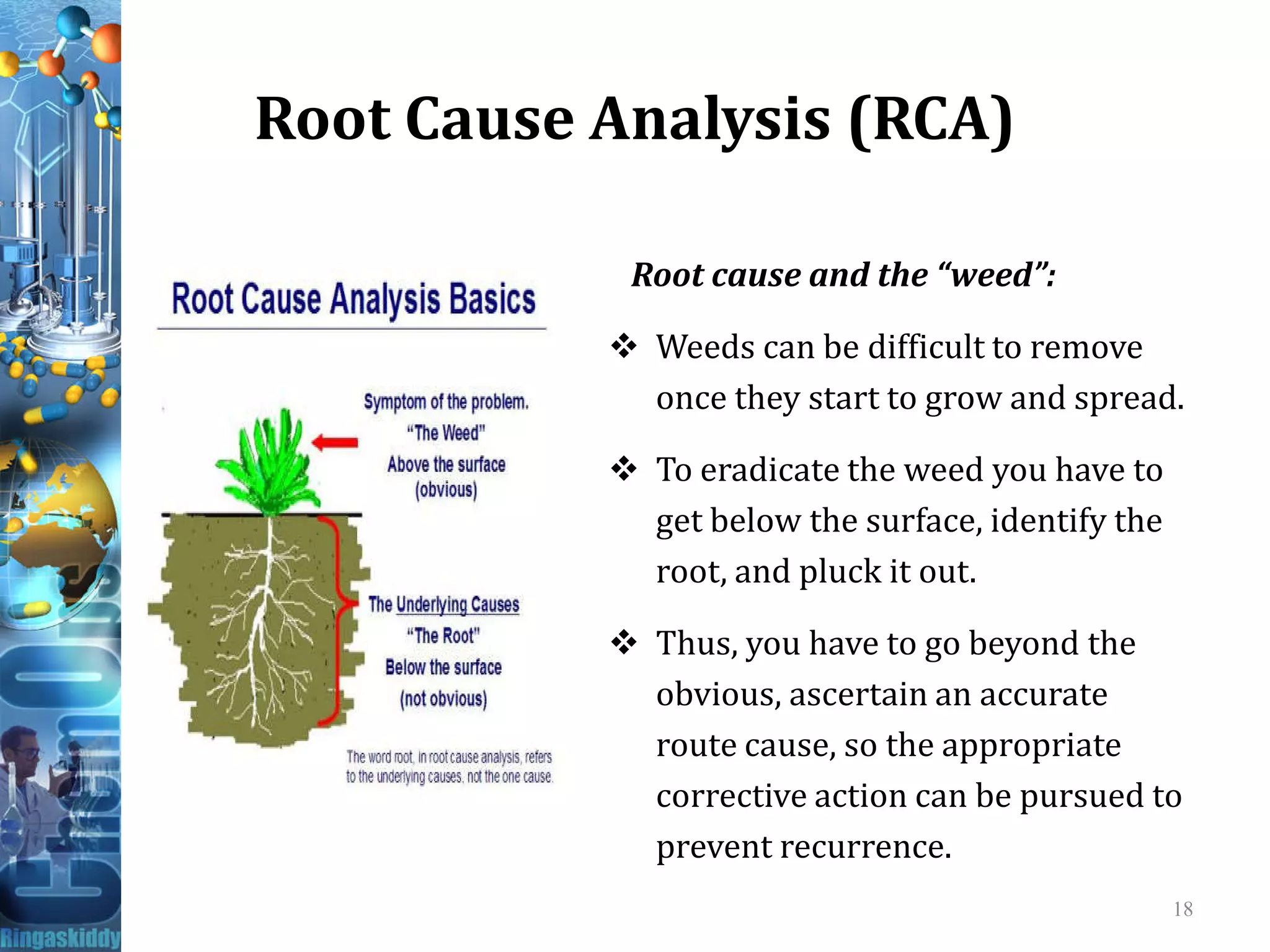
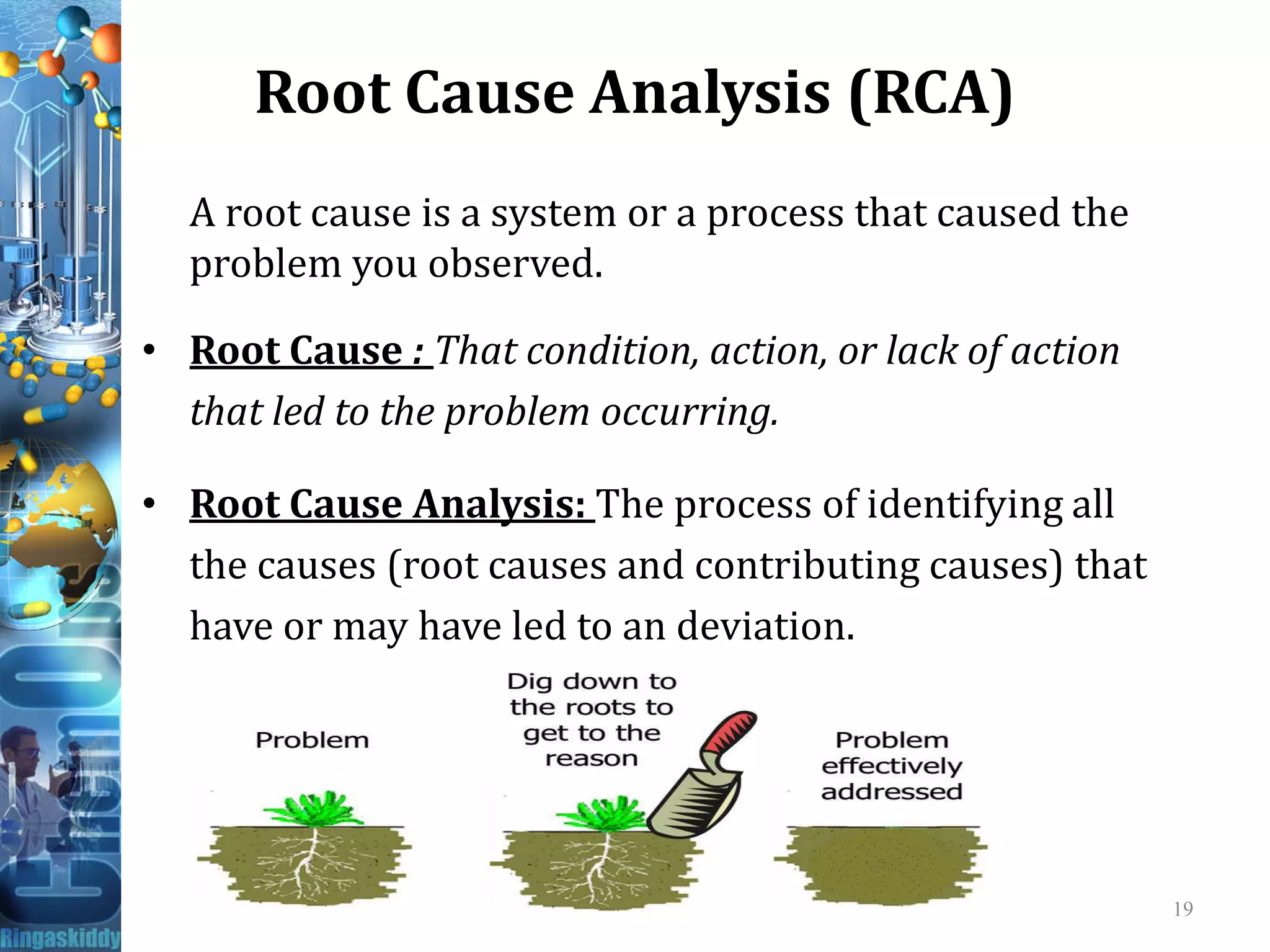

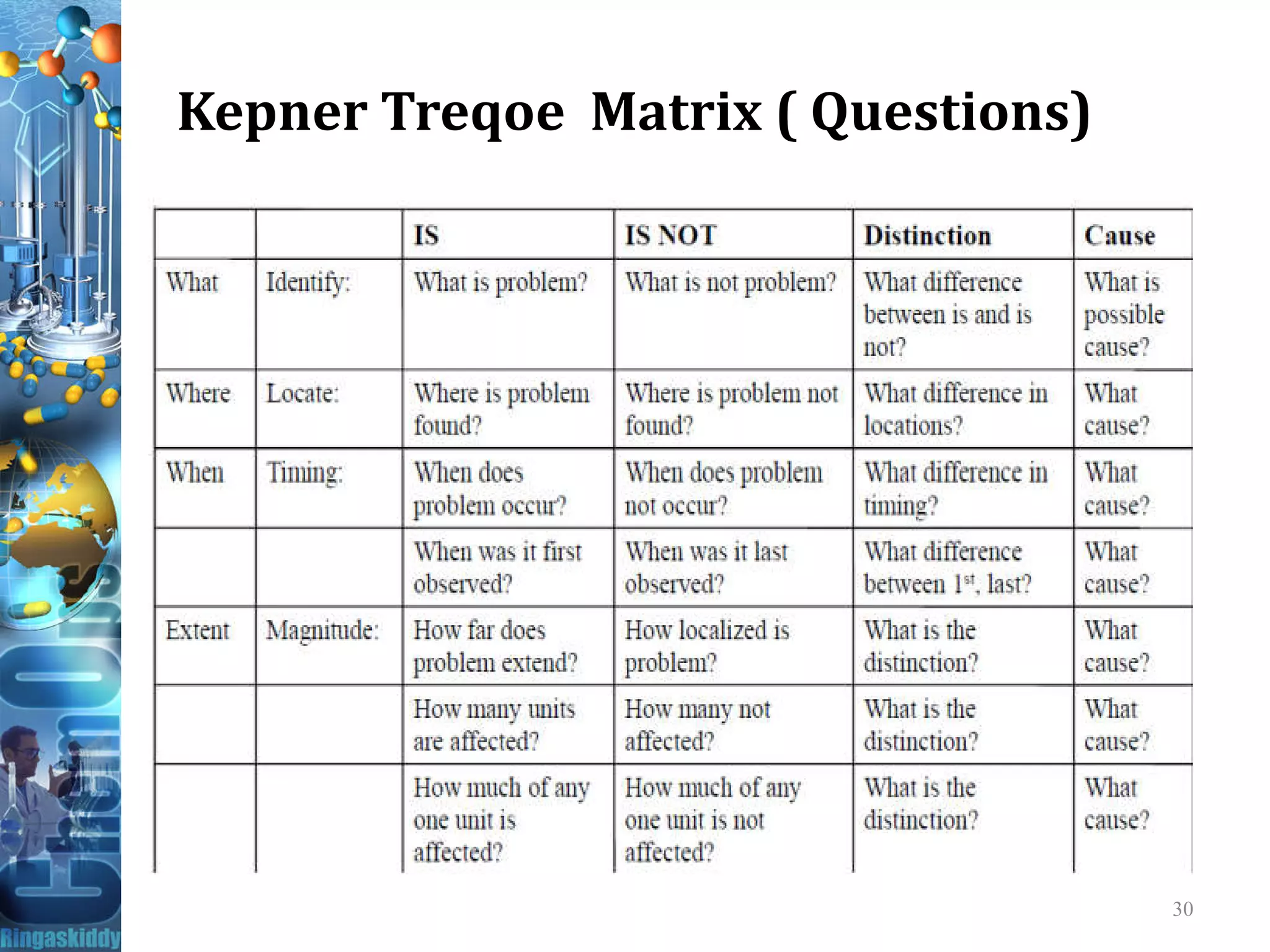





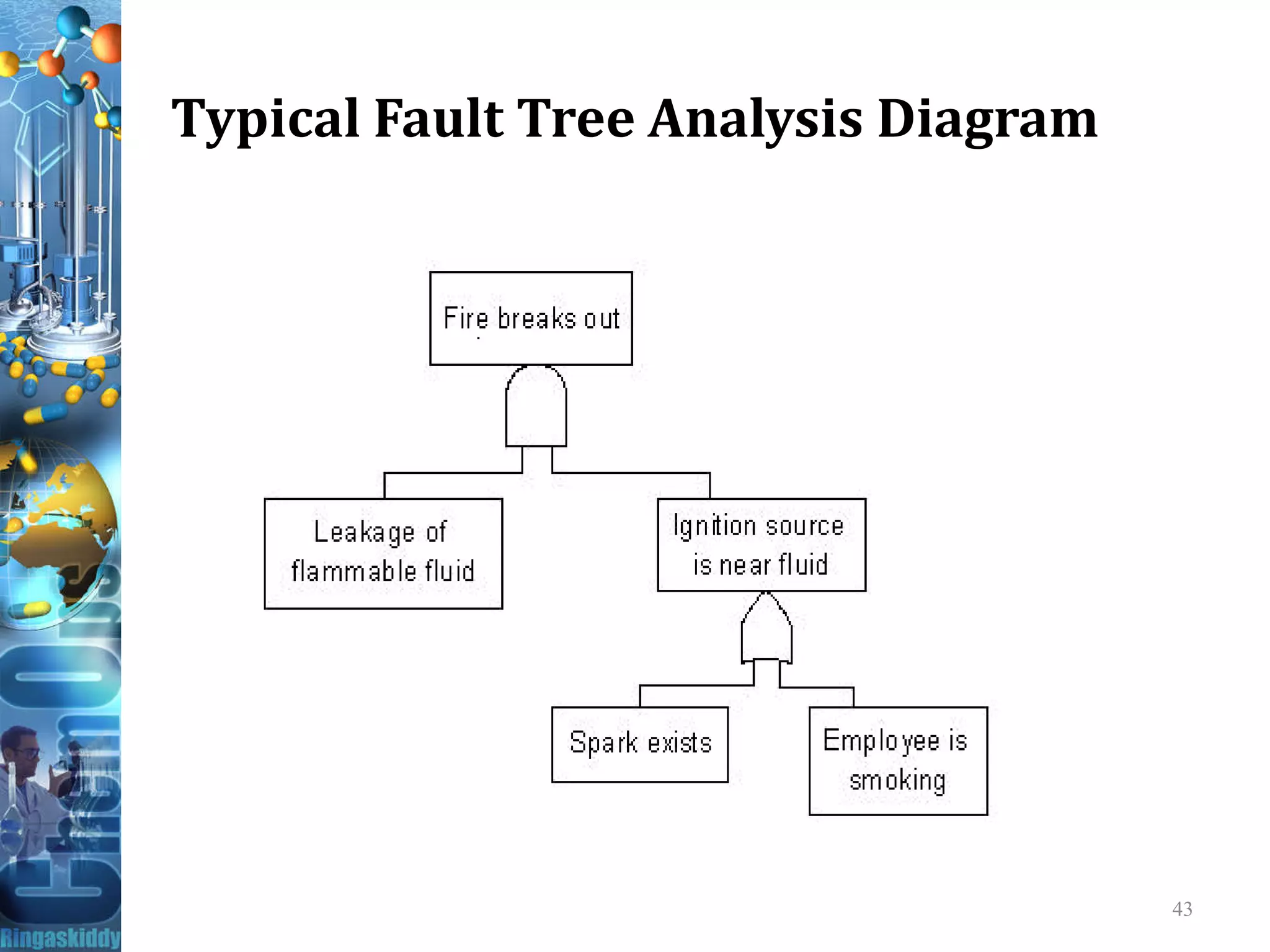






This document discusses deviation, out-of-specification (OOS), and complaint investigations and corrective and preventive action (CAPA). It defines key terms like nonconformity, corrective action, and preventive action. It describes the requirements for investigations per 21 CFR regulations. Common investigation tools like root cause analysis, 5 whys, fishbone diagrams, and fault tree analysis are explained. The document stresses identifying the root cause, avoiding focus on individuals, and verifying the effectiveness of CAPA.