Downloaded 12 times

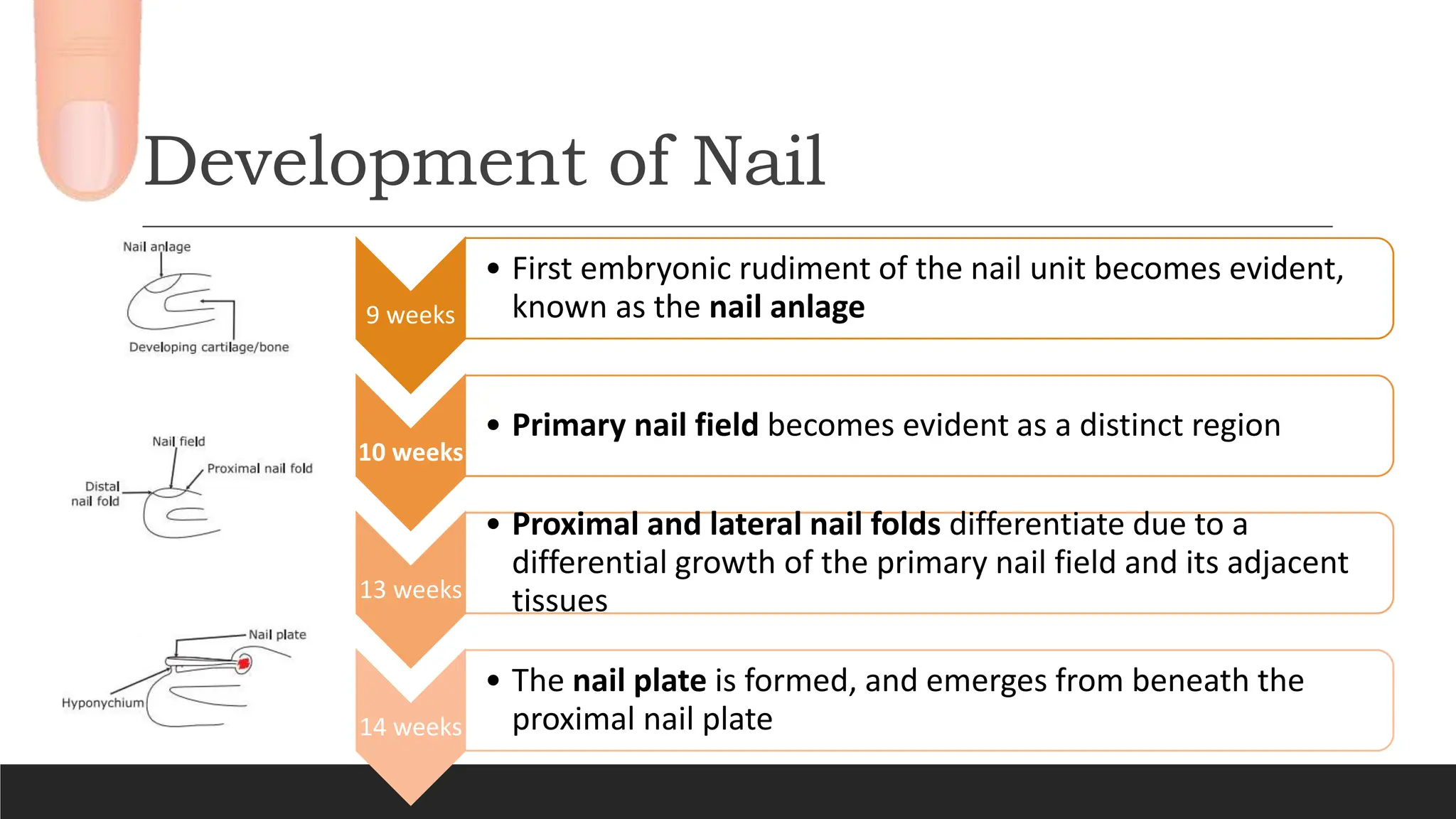
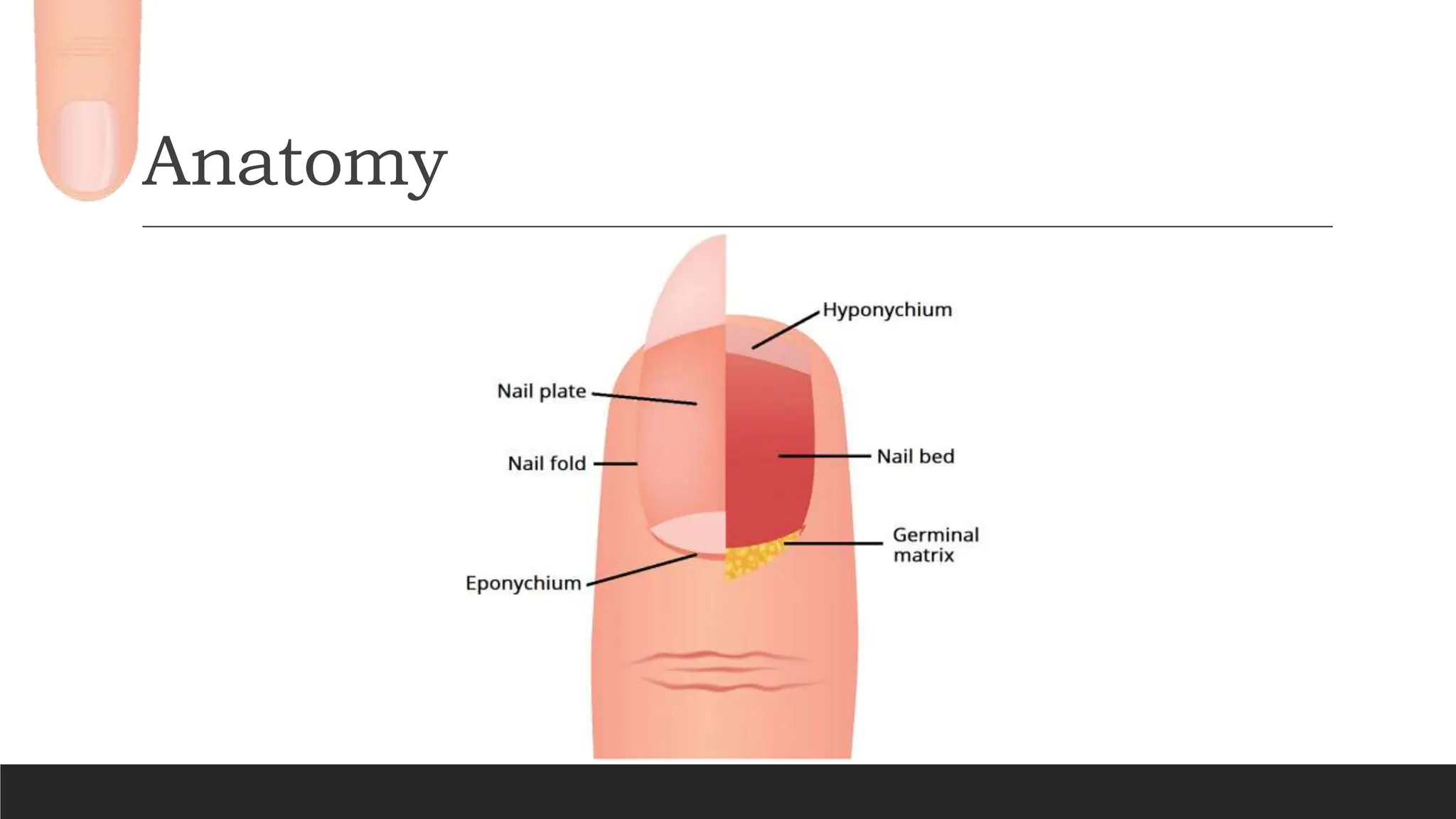
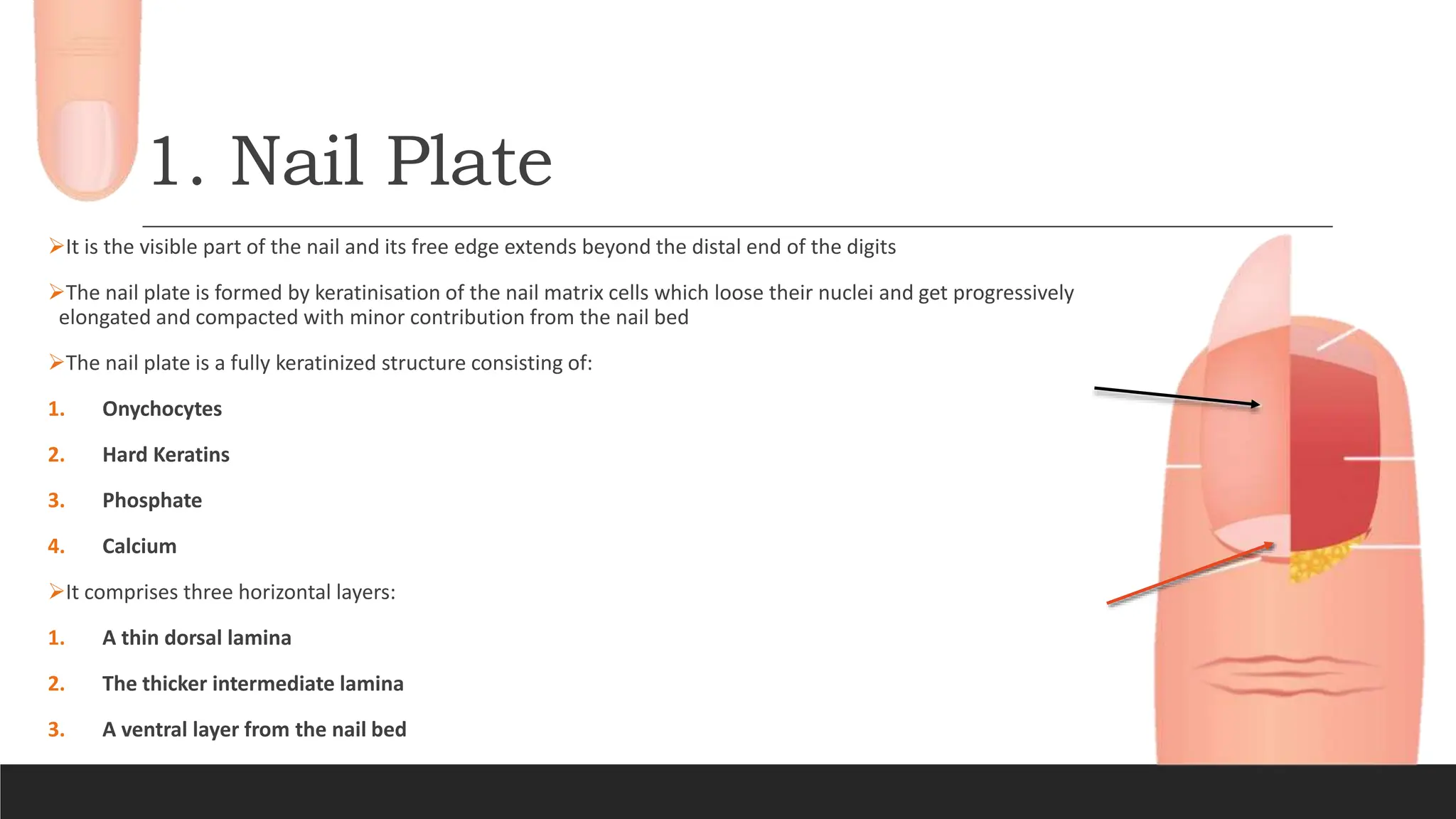
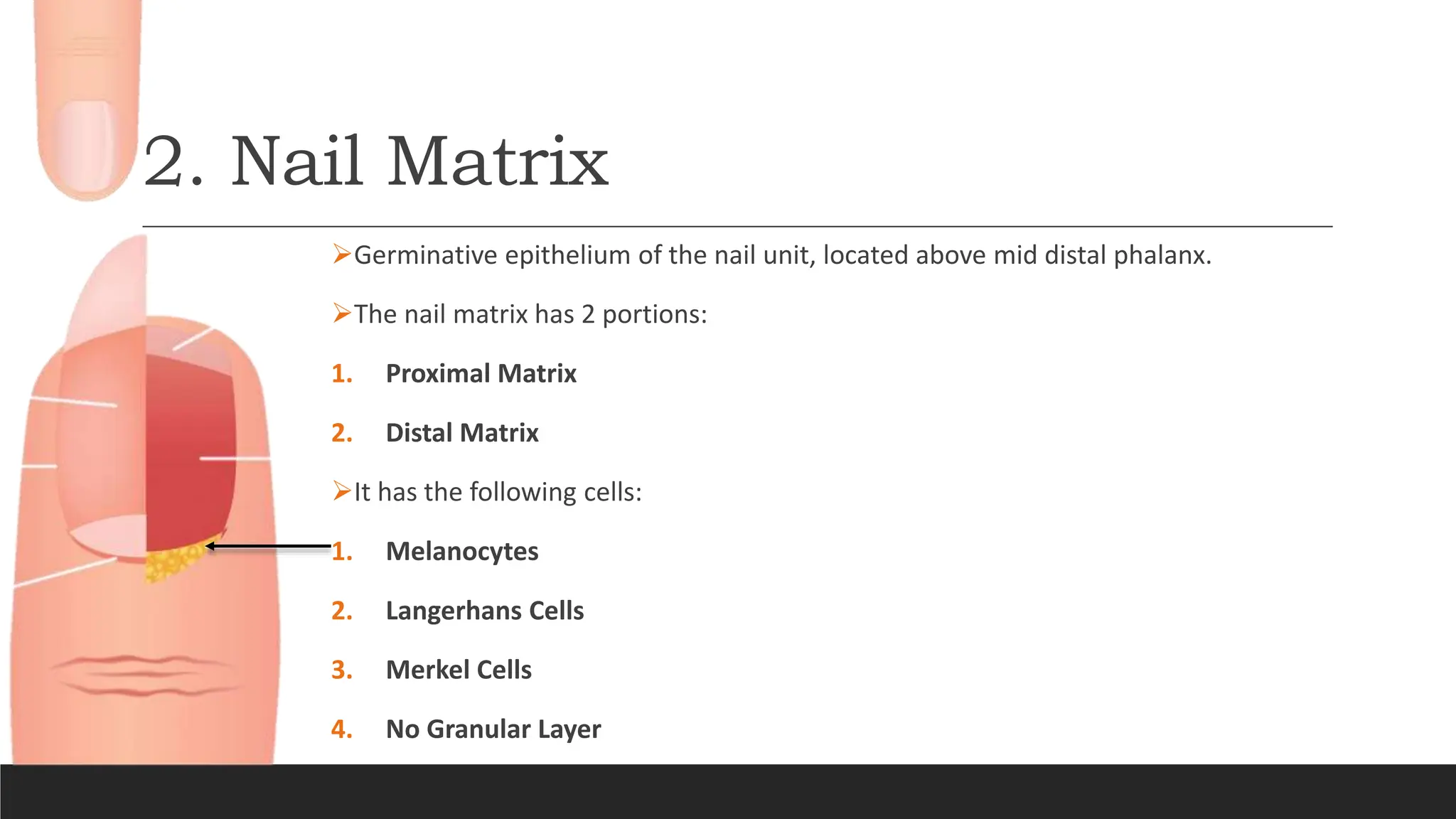
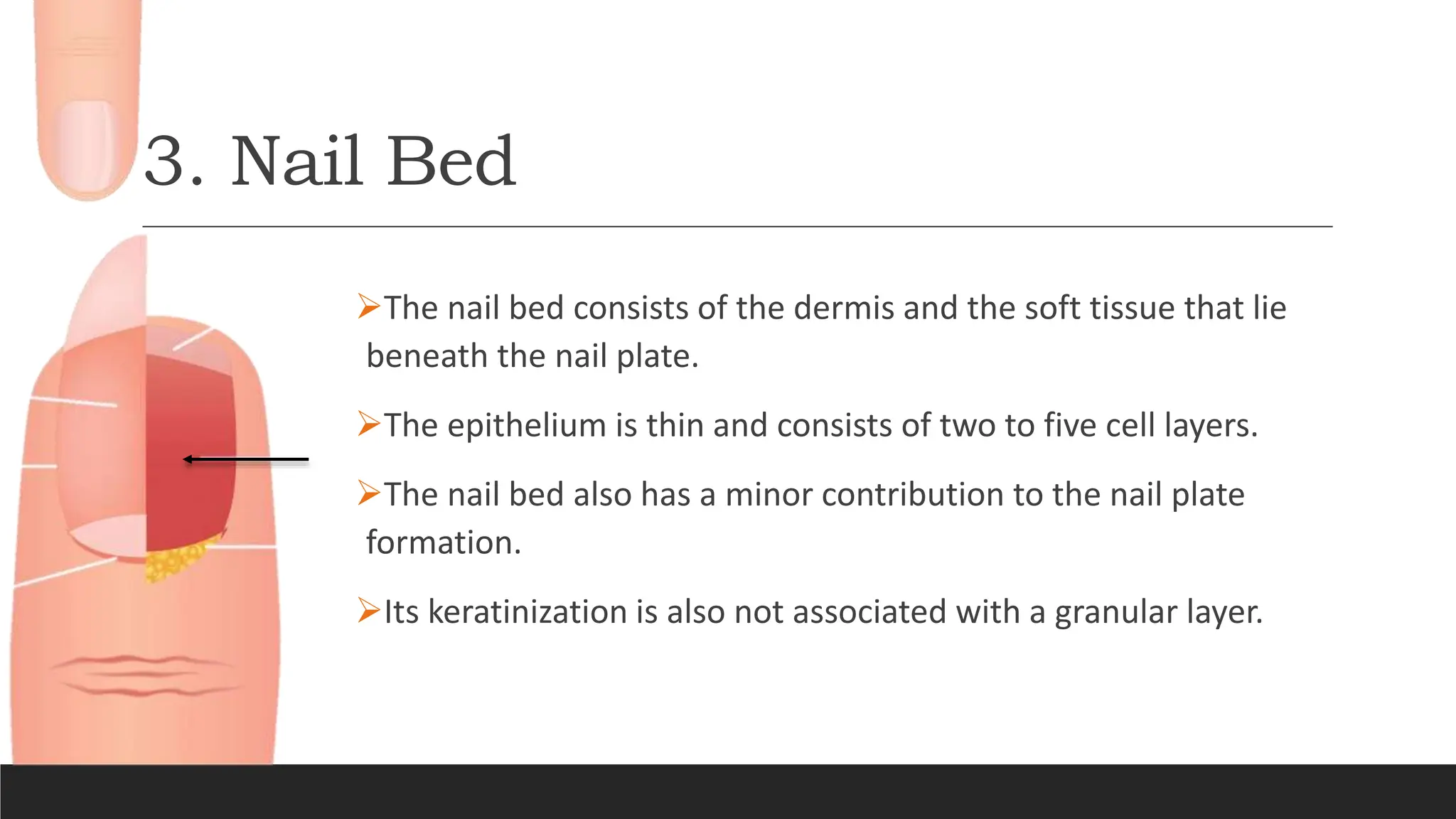
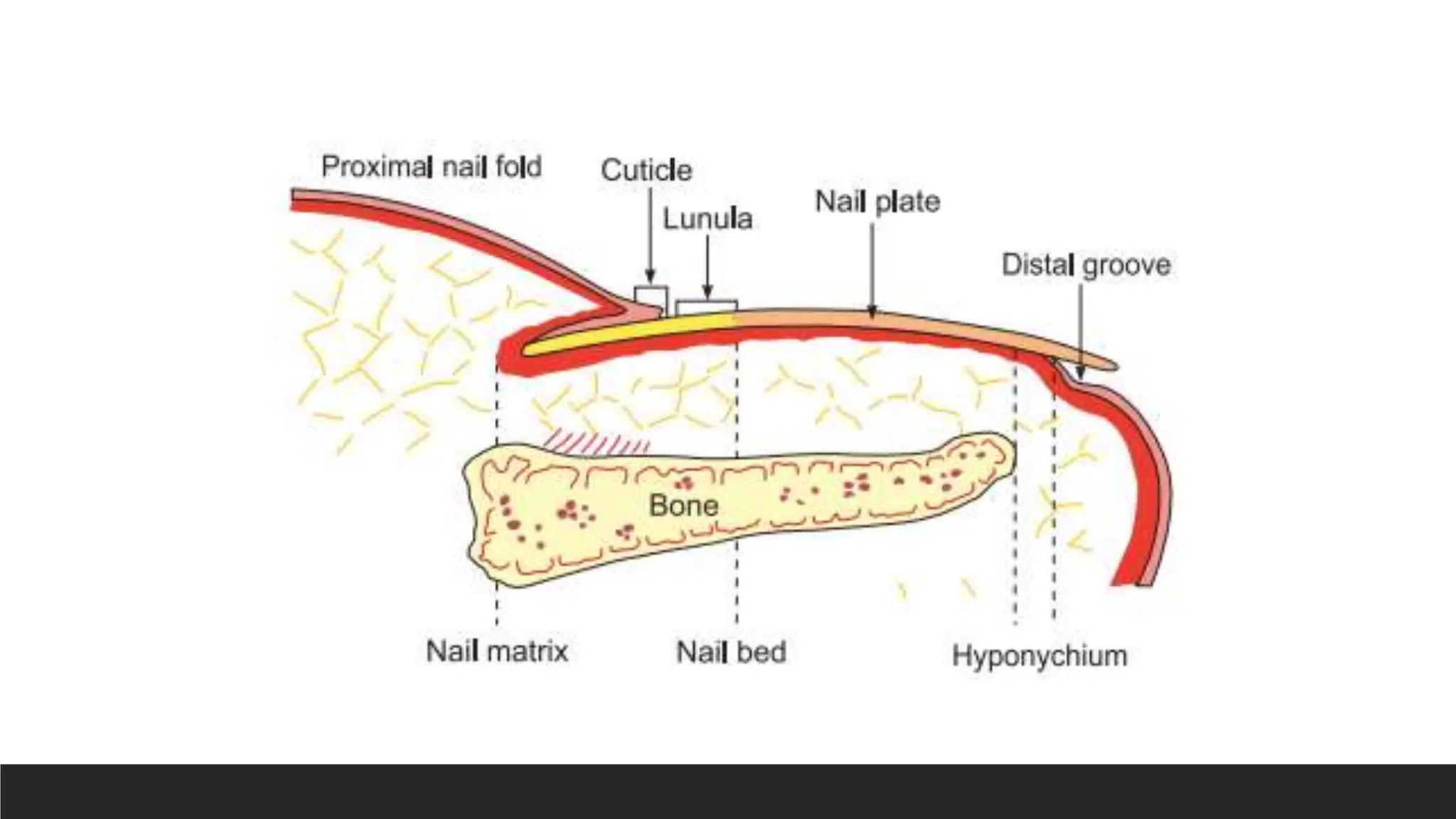

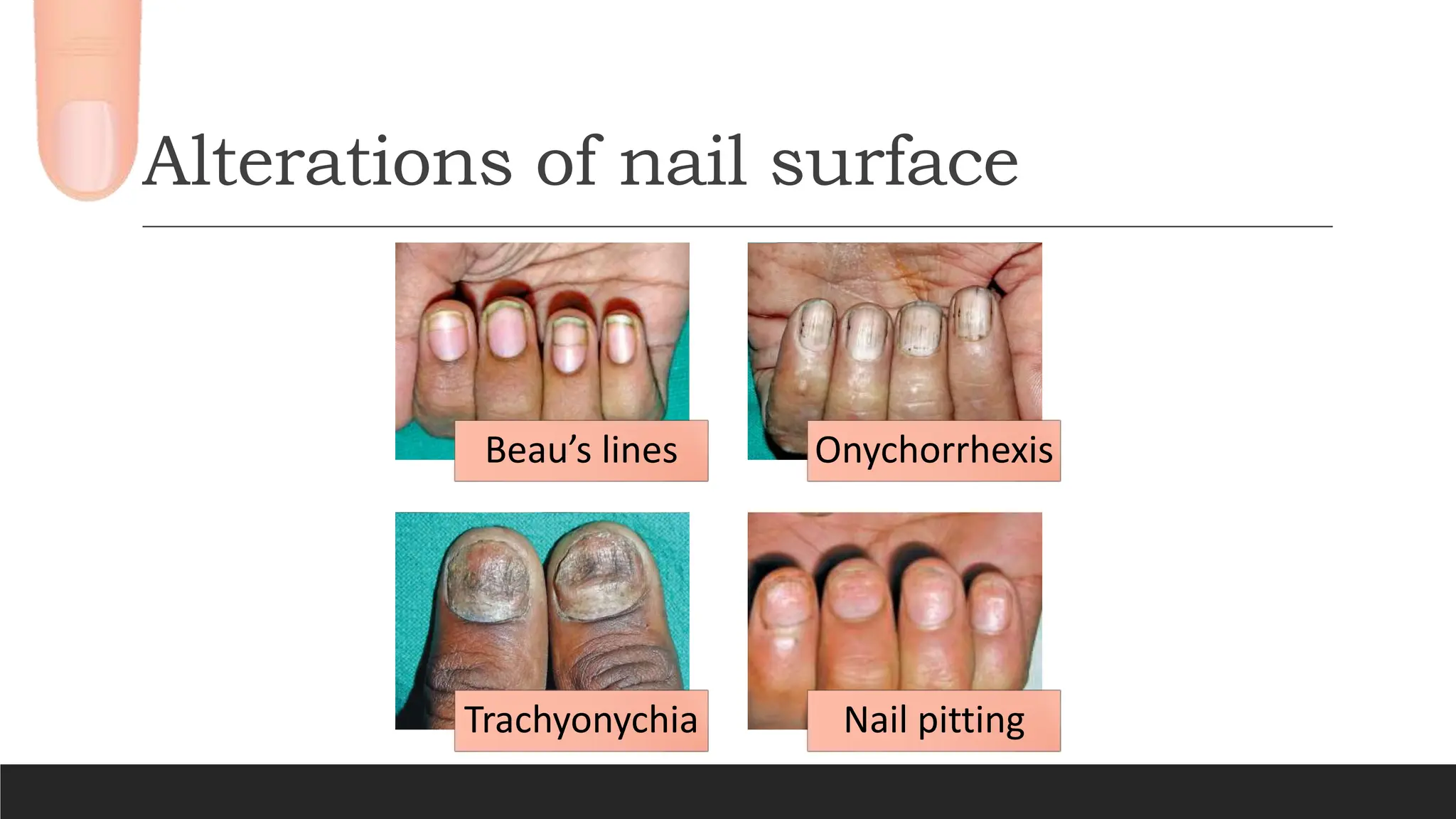
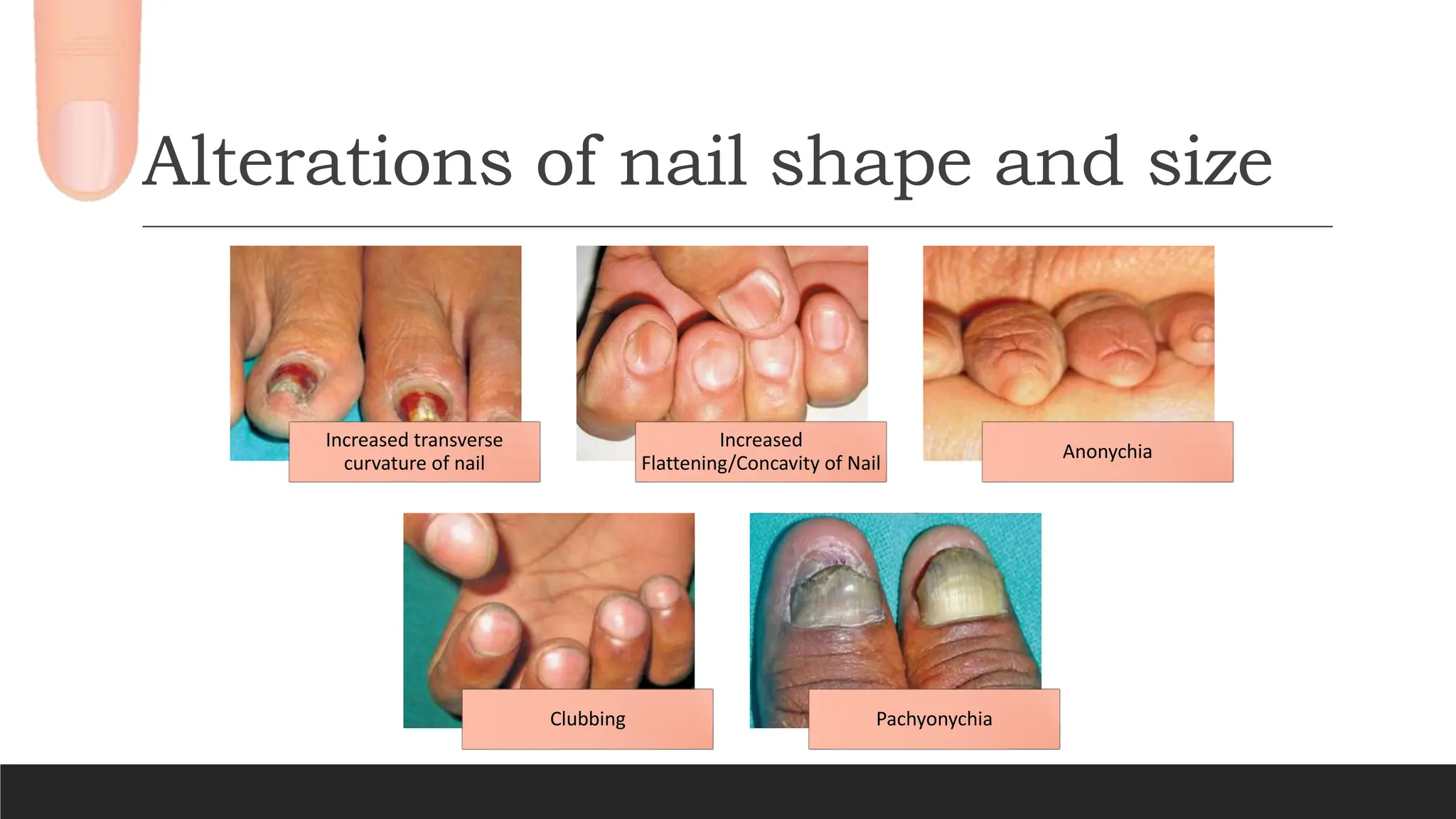
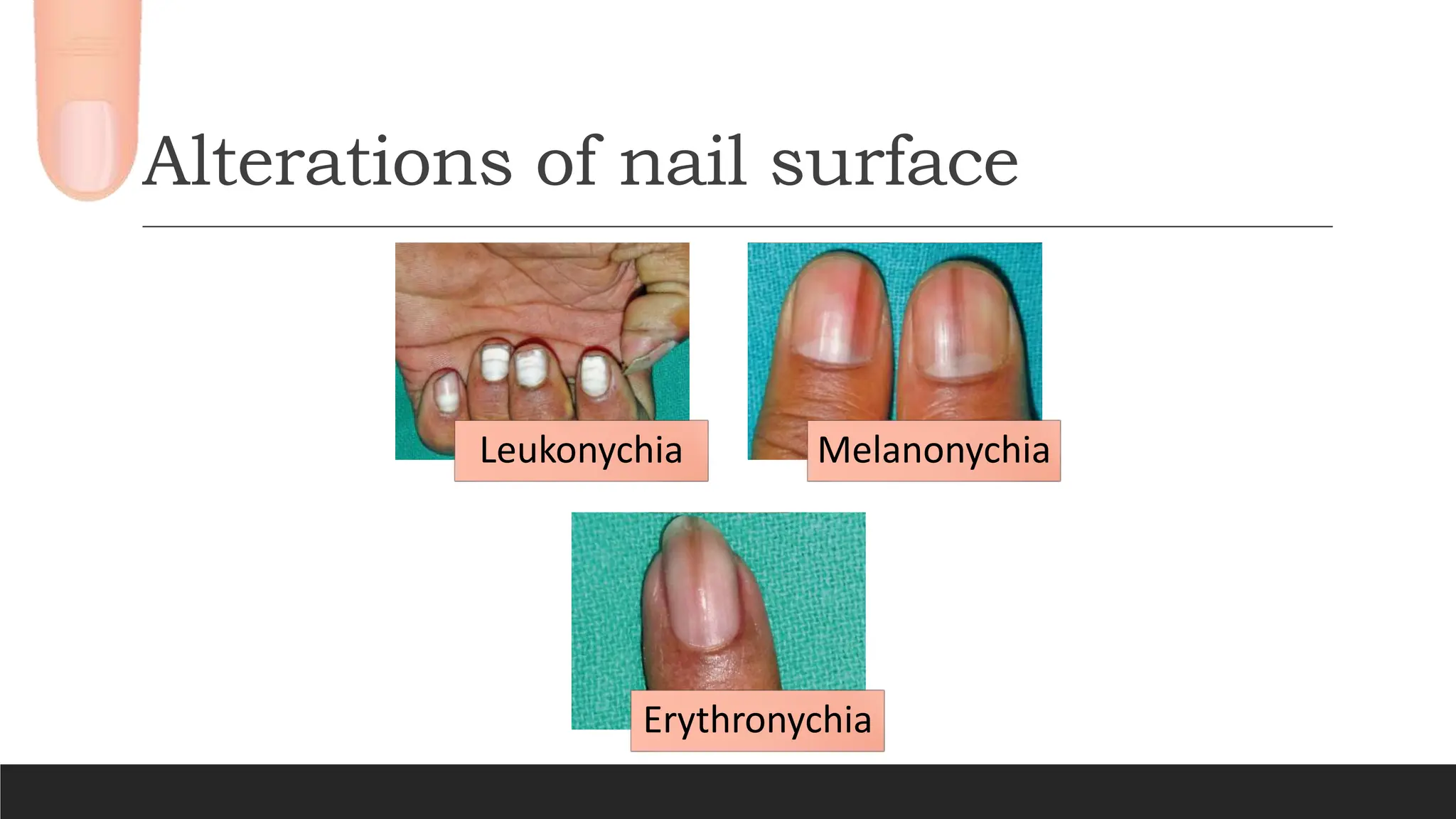
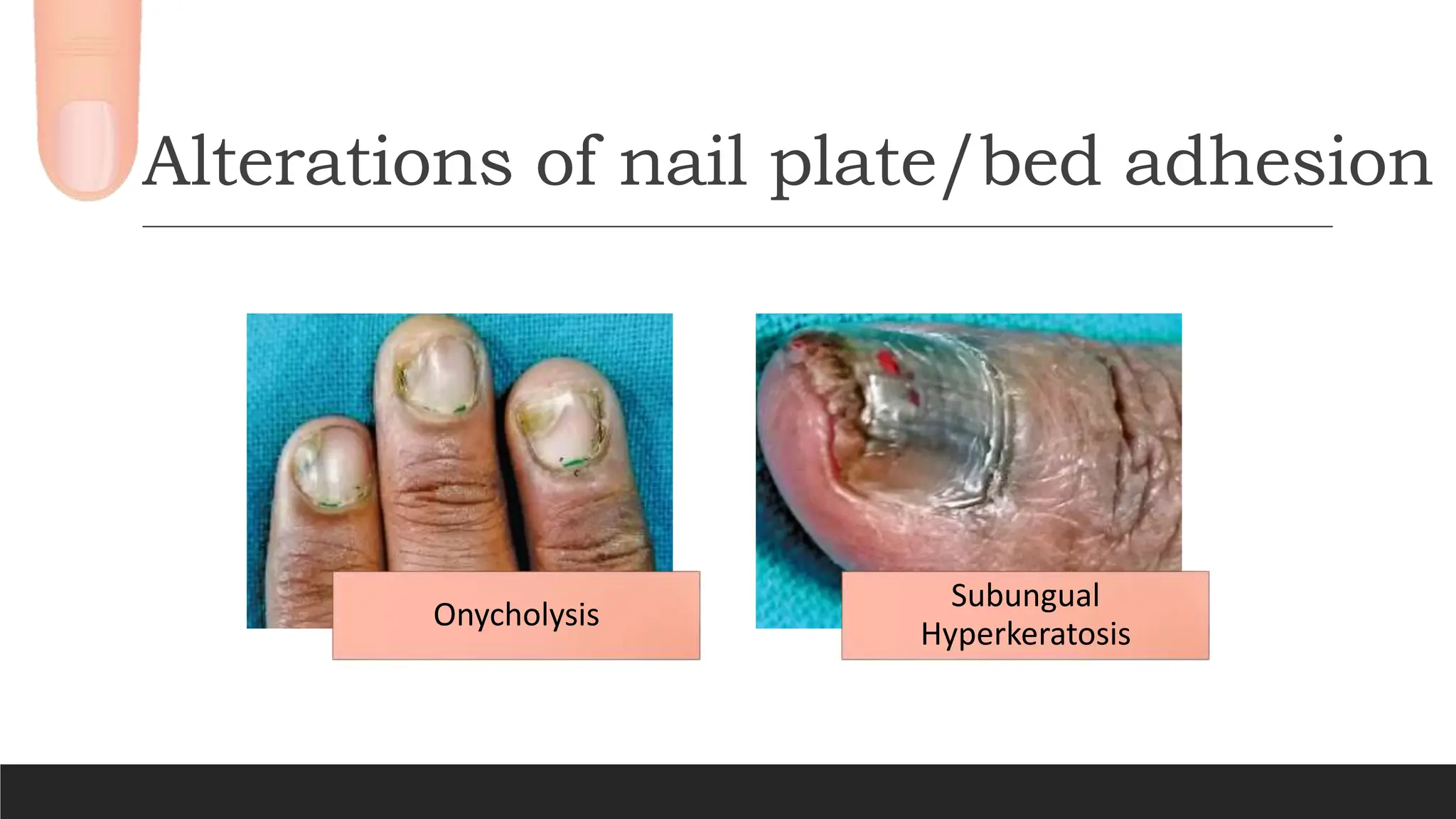


This document provides an overview of the structure and anatomy of the nail unit. It describes the key components of the nail including the nail plate, nail matrix, nail bed, eponychium, hyponychium, nail folds, and nail isthmus. It discusses the development, blood and nerve supply, growth, and functions of the nail. Finally, it outlines common nail signs that can be seen in health and disease such as Beau's lines, onychorrhexis, nail pitting, clubbing, and melanonychia.