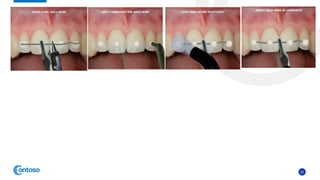
This case report describes the management of dental extrusion injuries in a 9-year-old female patient. Four teeth (31, 41, 42, 11, 21) were severely extruded or avulsed following a bicycle accident. The extruded teeth had fully formed roots and closed apices. The teeth were repositioned and splinted. Two avulsed teeth received endodontic treatment after replantation. The patient was followed clinically and radiographically for 18 months. Three of the extruded teeth responded to sensitivity tests after 12 months, while one tooth remained unresponsive but asymptomatic. The case demonstrates that pulps of traumatized teeth with closed apices may remain vital and monitoring is important to avoid unnecessary