Downloaded 57 times








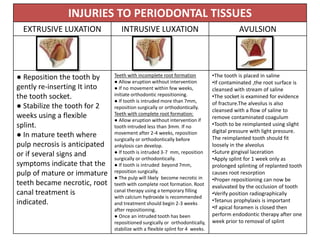





The document discusses traumatic dental injuries (TDI), their prevalence, causes, and classifications of injury types. It details emergency and non-emergency management treatments for various dental injuries, emphasizing the importance of prompt dental care and specific protocols for managing displaced, fractured, and avulsed teeth. Additionally, it highlights the psychological aspects and common misconceptions among the public regarding dental injuries.























































































