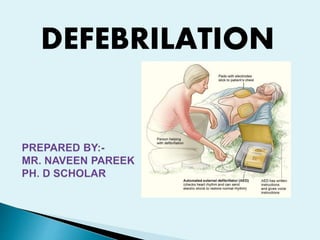



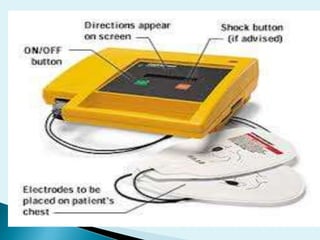


This document discusses defibrillation, which is a treatment used to restore normal heart rhythm in patients experiencing ventricular fibrillation or pulseless ventricular tachycardia. It defines defibrillation and describes the different types of defibrillators, including manual external defibrillators, automated external defibrillators, implantable cardioverter defibrillators, and wearable cardiac defibrillators. It also covers how defibrillation works, the precautions that must be taken with the procedure, and the risks involved.












































































