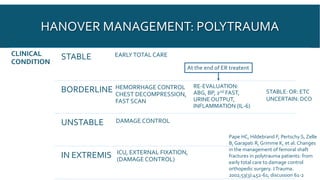
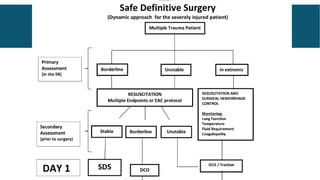
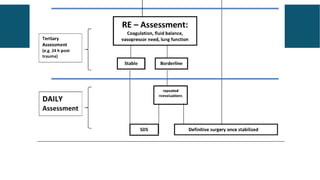
Damage control orthopedics (DCO) is an approach for treating severely injured polytrauma patients to avoid worsening their unstable condition from additional surgical stress. It involves early stabilization of fractures through temporary external or minimal internal fixation to be followed later by definitive treatment after the patient's physiology is stabilized. While early total care was previously favored, DCO is now widely accepted for polytrauma patients as it decreases systemic complications by limiting the "second hit" effect compared to prolonged definitive surgeries. The approach and timing of DCO versus early total care must be individualized based on the patient's clinical status and injury pattern.