

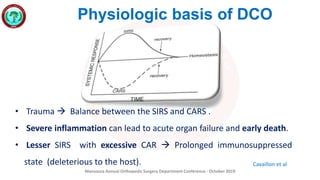





The document discusses the principles and applications of Damage Control Orthopedics (DCO) as presented at the Mansoura Annual Orthopedic Surgery Department Conference in October 2019. DCO focuses on stabilizing orthopedic injuries and optimizing patient physiology, emphasizing the importance of early intervention and coordination with trauma surgery to prevent severe inflammatory responses. Key topics include the management of polytrauma patients, resuscitation strategies, and guidelines for surgical intervention following injury.

















































































