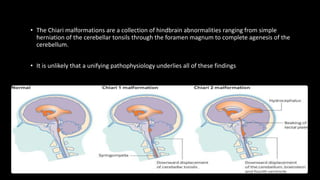
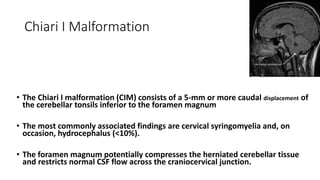
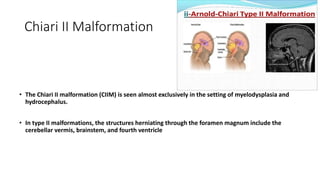
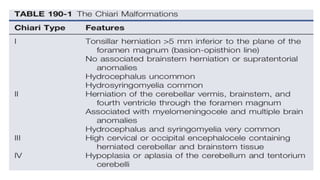
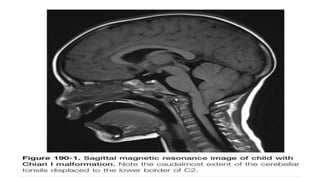
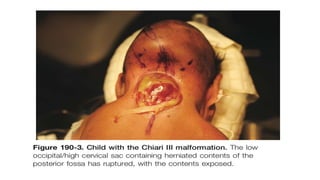
Chiari malformations are a set of hindbrain abnormalities characterized by cerebellar herniation, with Chiari I and II being the most common types. The clinical presentation varies widely, affecting cerebrospinal fluid flow and leading to symptoms like headaches and neurological disturbances. Surgical decompression is the primary treatment for symptomatic patients, emphasizing the need for proper patient selection and assessment of cranial physiology.