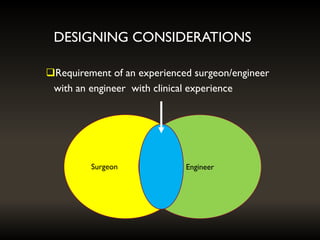
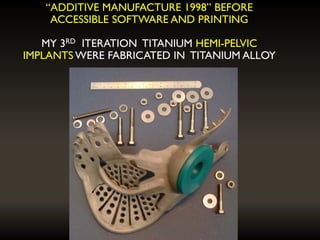
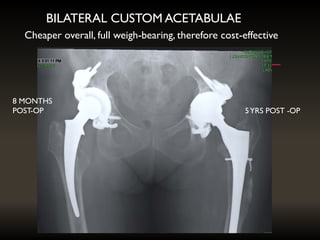
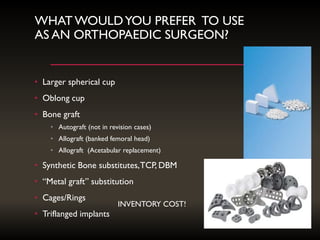
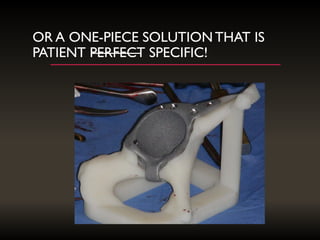
The document discusses the use and future potential of custom implants in orthopaedic surgery, highlighting their benefits in reducing inventory costs and improving surgical outcomes through personalized design. It emphasizes the importance of collaboration between surgeons and engineers, the need for better materials, and adherence to biological principles to avoid implant failures. Additionally, it notes the increasing viability of custom implants due to advancements in 3D printing technology and the continuous evolution of implant designs.