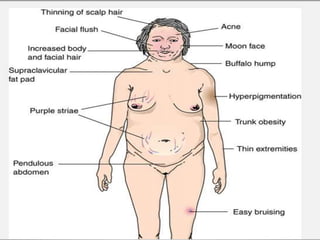
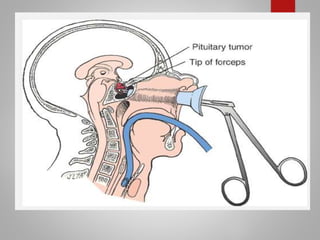
Cushing's syndrome is caused by prolonged high levels of the hormone cortisol and results in weight gain, high blood pressure, and other signs. It can be caused by pituitary or adrenal tumors that overproduce cortisol or related hormones. Diagnosis involves blood and urine tests showing elevated cortisol levels. Treatment options include surgery to remove the tumor, medications to suppress cortisol production, and lifelong hormone replacement after adrenal removal. Nursing care focuses on managing skin integrity issues, assisting with self-care due to weakness, addressing changes in body image and mood, and providing postoperative monitoring and care.














































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









