
Downloaded 192 times
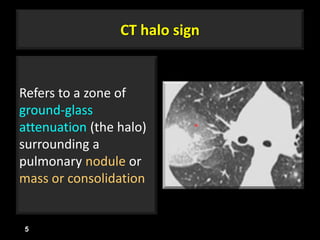
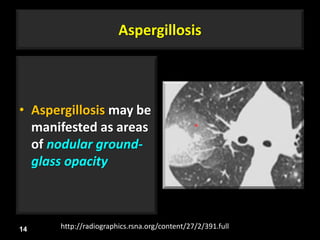

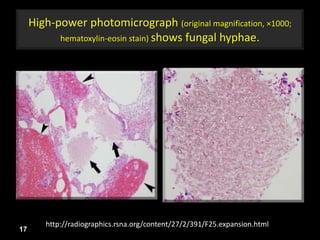
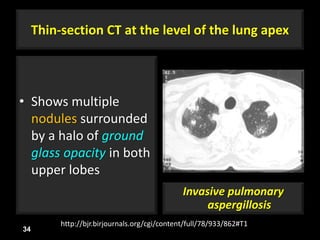
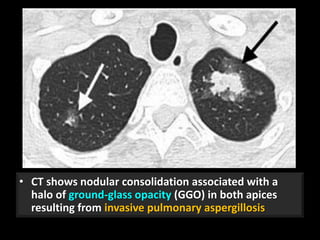
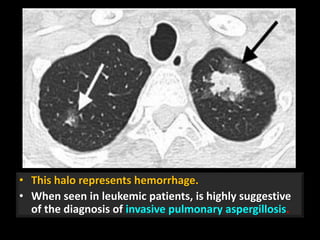
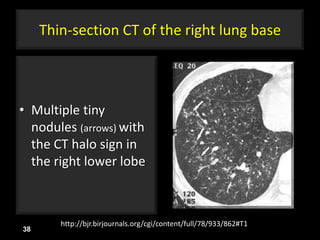
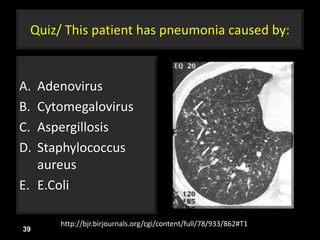
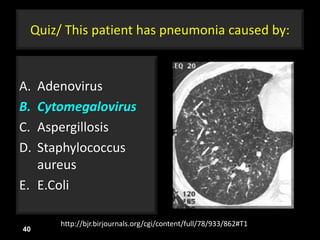
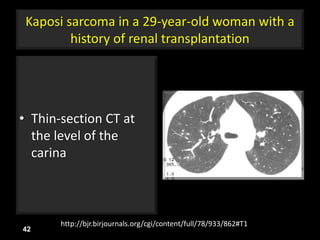
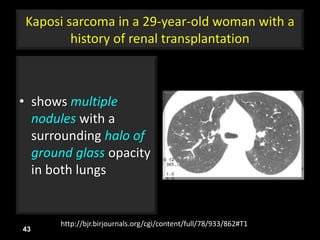
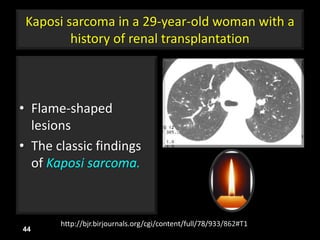
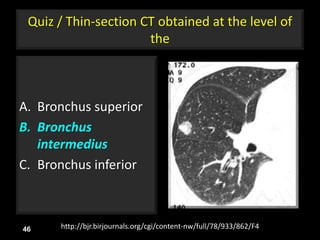
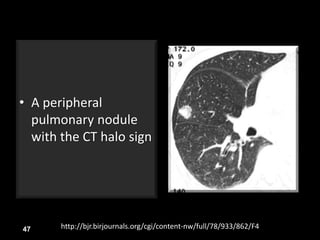
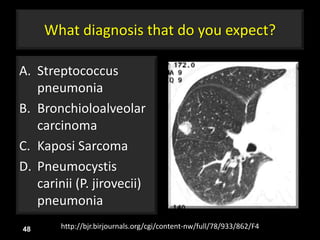
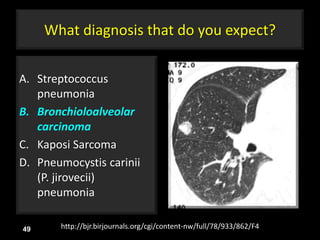

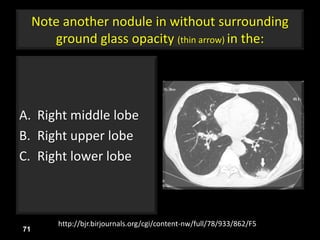
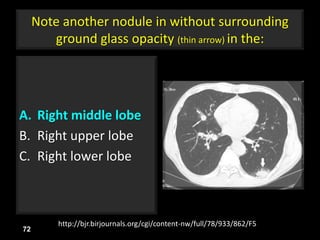
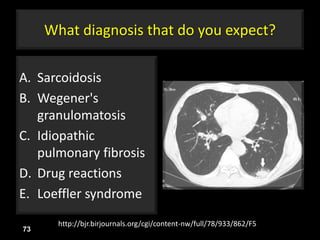
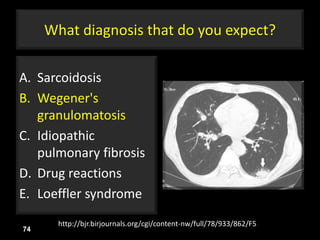
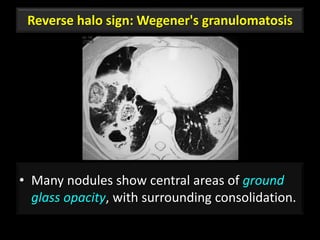
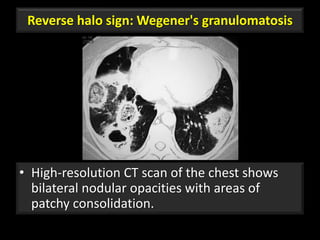
This document is a presentation on CT halo sign by Dr. Mazen Qusaibaty. It discusses what the CT halo sign refers to and provides examples of diseases that can present with the halo sign, including aspergillosis, eosinophilic pneumonia, bronchiolitis obliterans with organizing pneumonia, and others. Specific case examples are presented to illustrate the halo sign in diseases such as invasive pulmonary aspergillosis, Kaposi sarcoma, and eosinophilic pneumonia. The histological features underlying the halo sign are also described for different conditions.
































































































