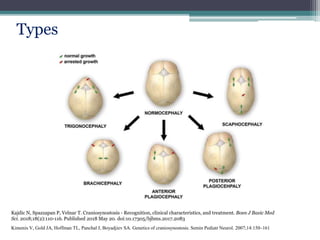
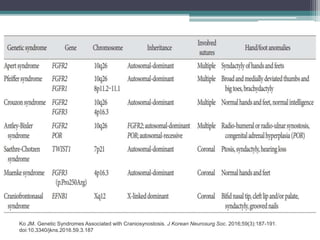
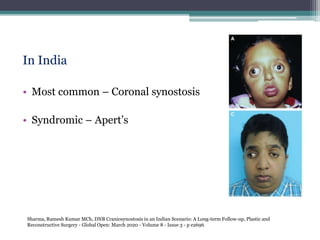
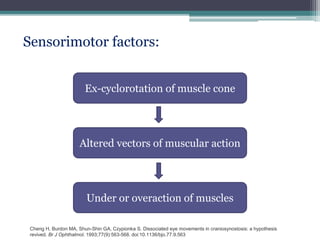
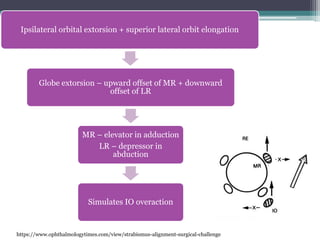
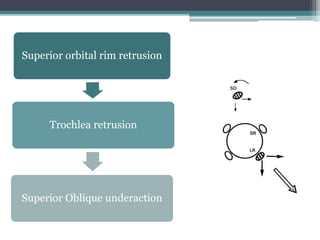
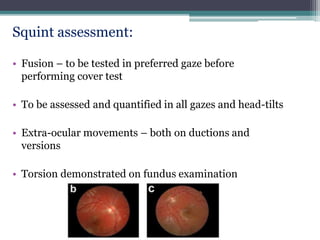
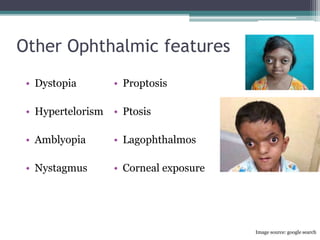
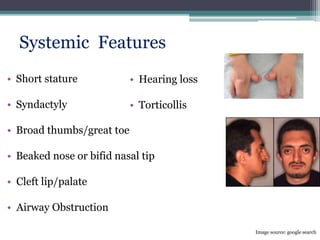
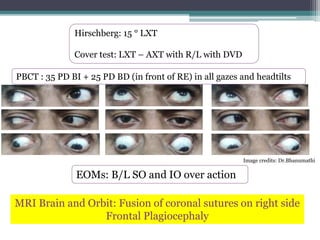
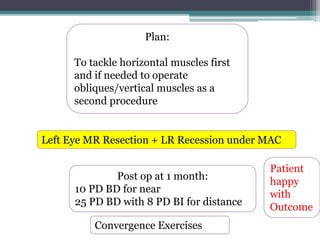
Strabismus is common in patients with craniosynostosis. The document discusses craniosynostosis, the various types and causes. Strabismus in craniosynostosis can be due to anatomical abnormalities of the orbits and extraocular muscles as well as sensorimotor factors. Evaluation involves a thorough eye examination and imaging. Management includes amblyopia treatment, craniofacial surgery, and strabismus surgery which can be challenging due to anatomical variations. Two case examples are presented of patients with plagiocephaly who presented with superior oblique muscle abnormalities but responded well to inferior oblique weakening procedures. Proper evaluation and customized surgical planning is important for achieving good outcomes in strabism
































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





