Download as PDF, PPTX



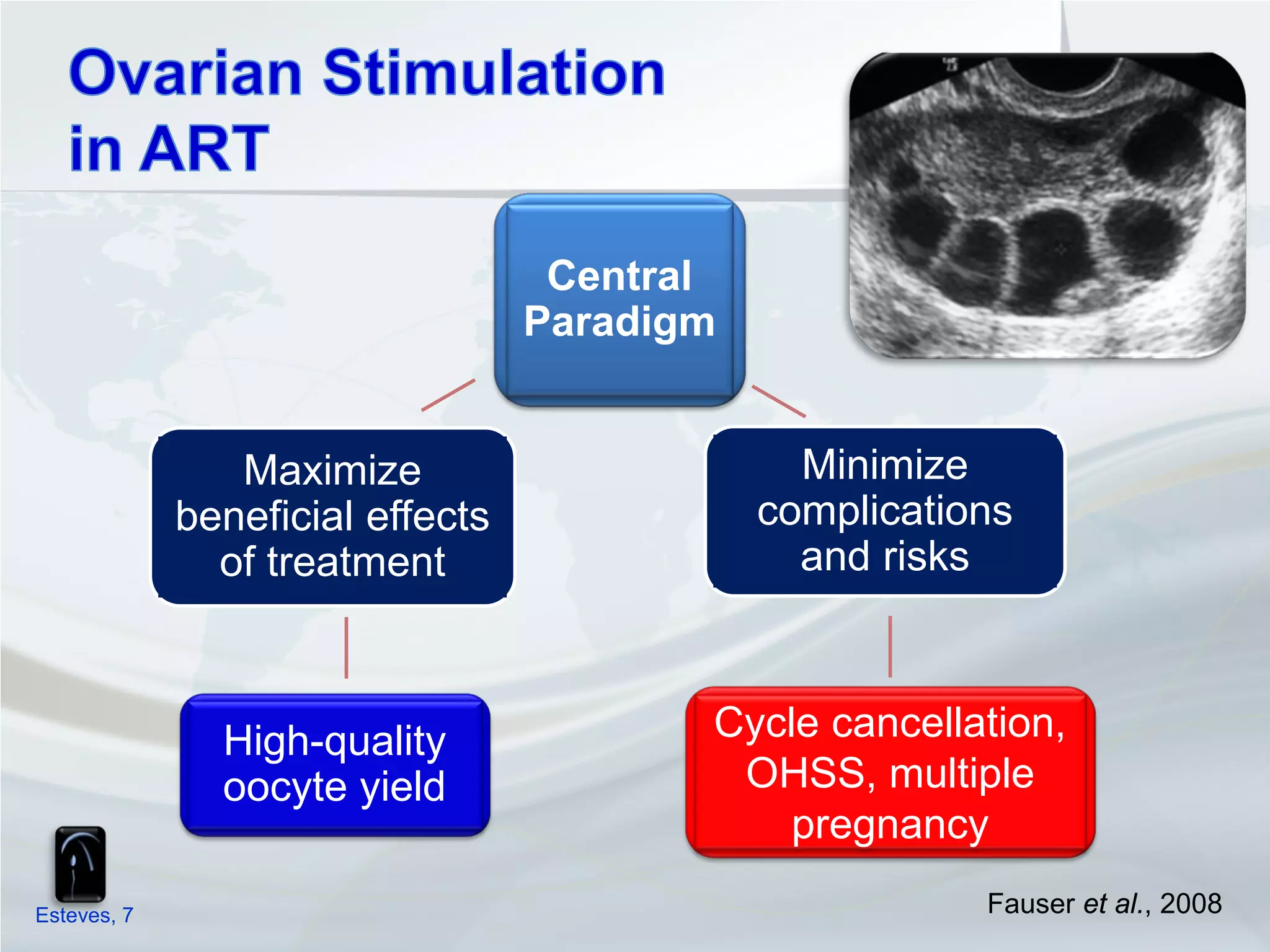
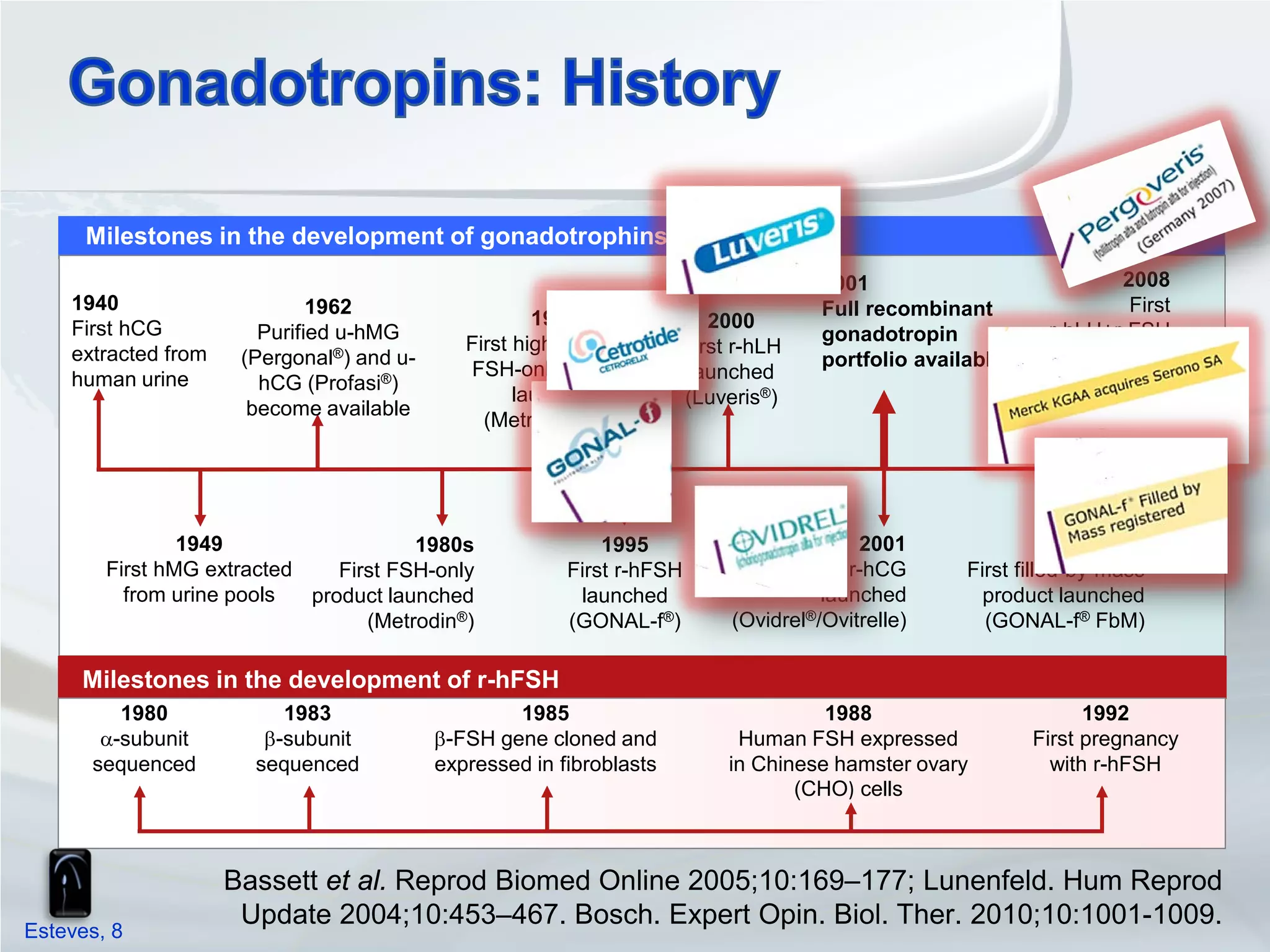
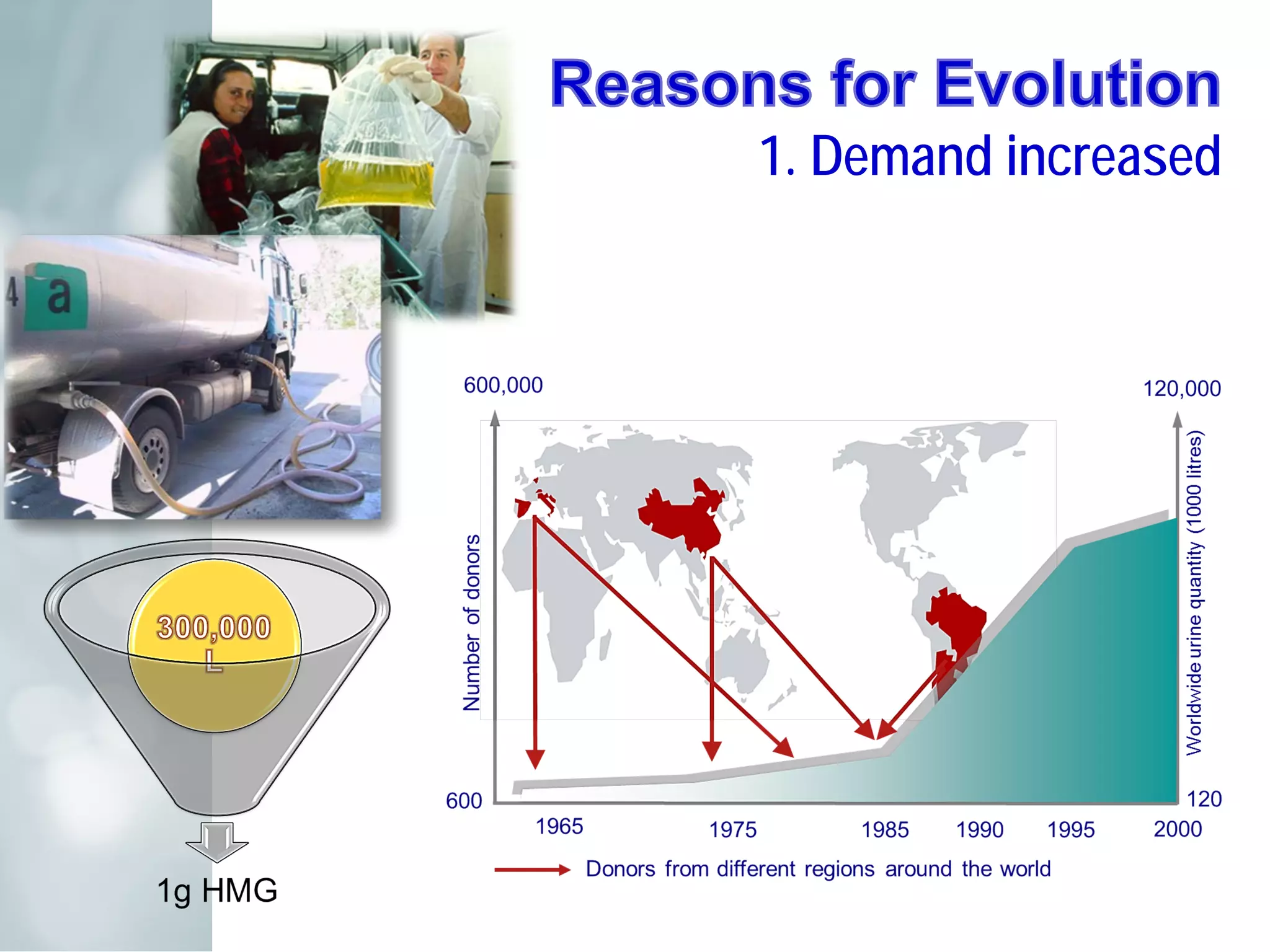
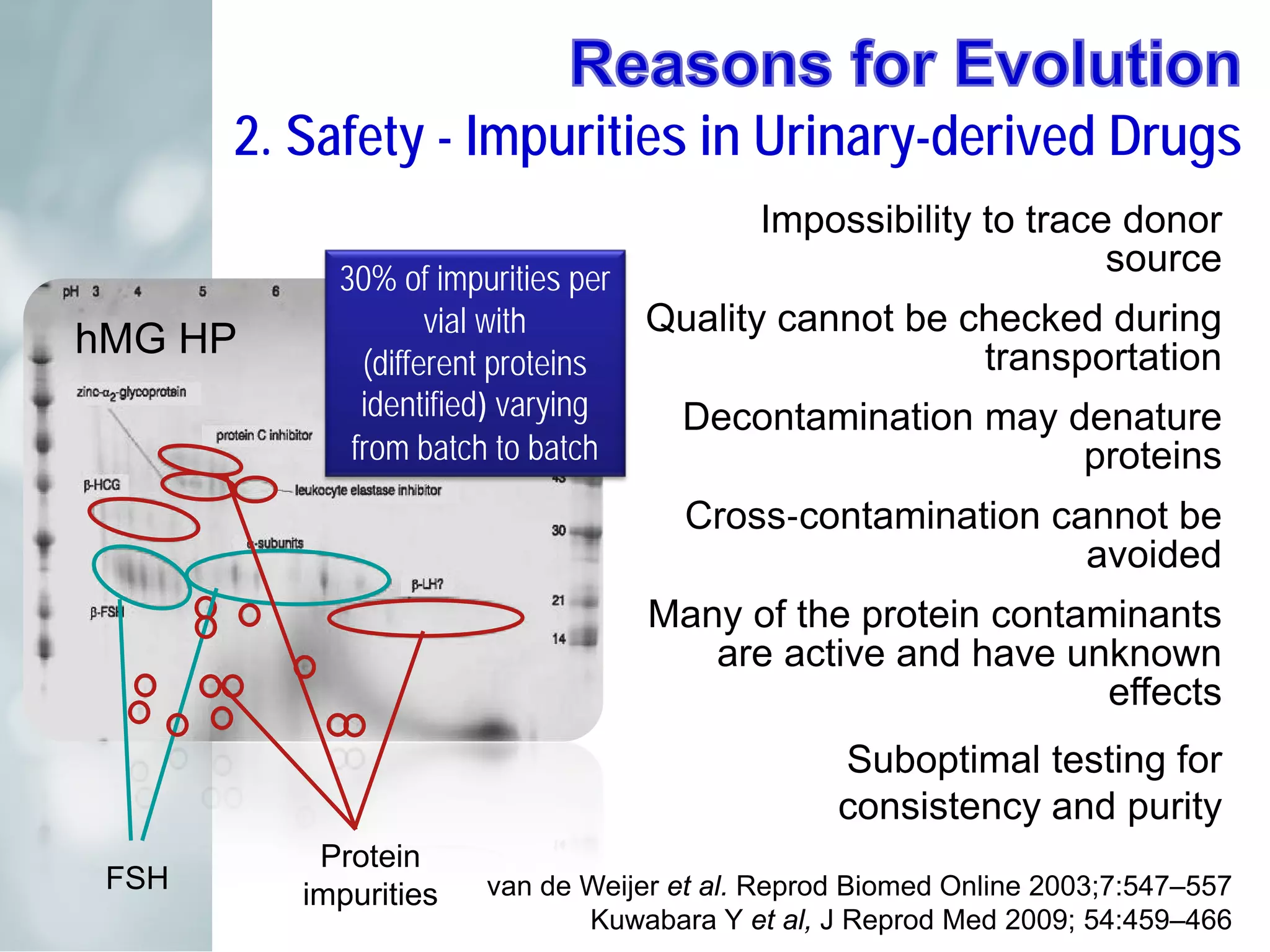
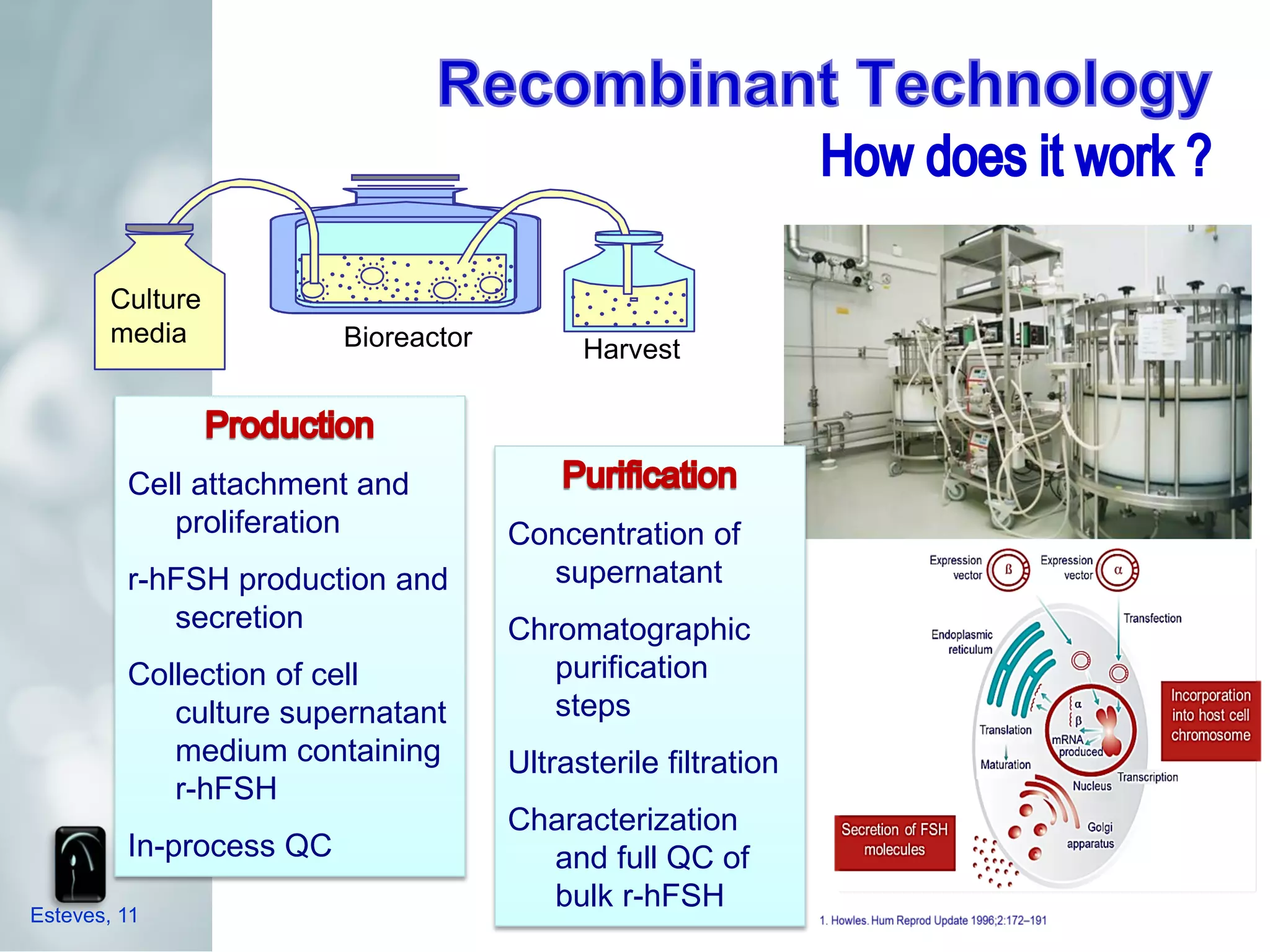
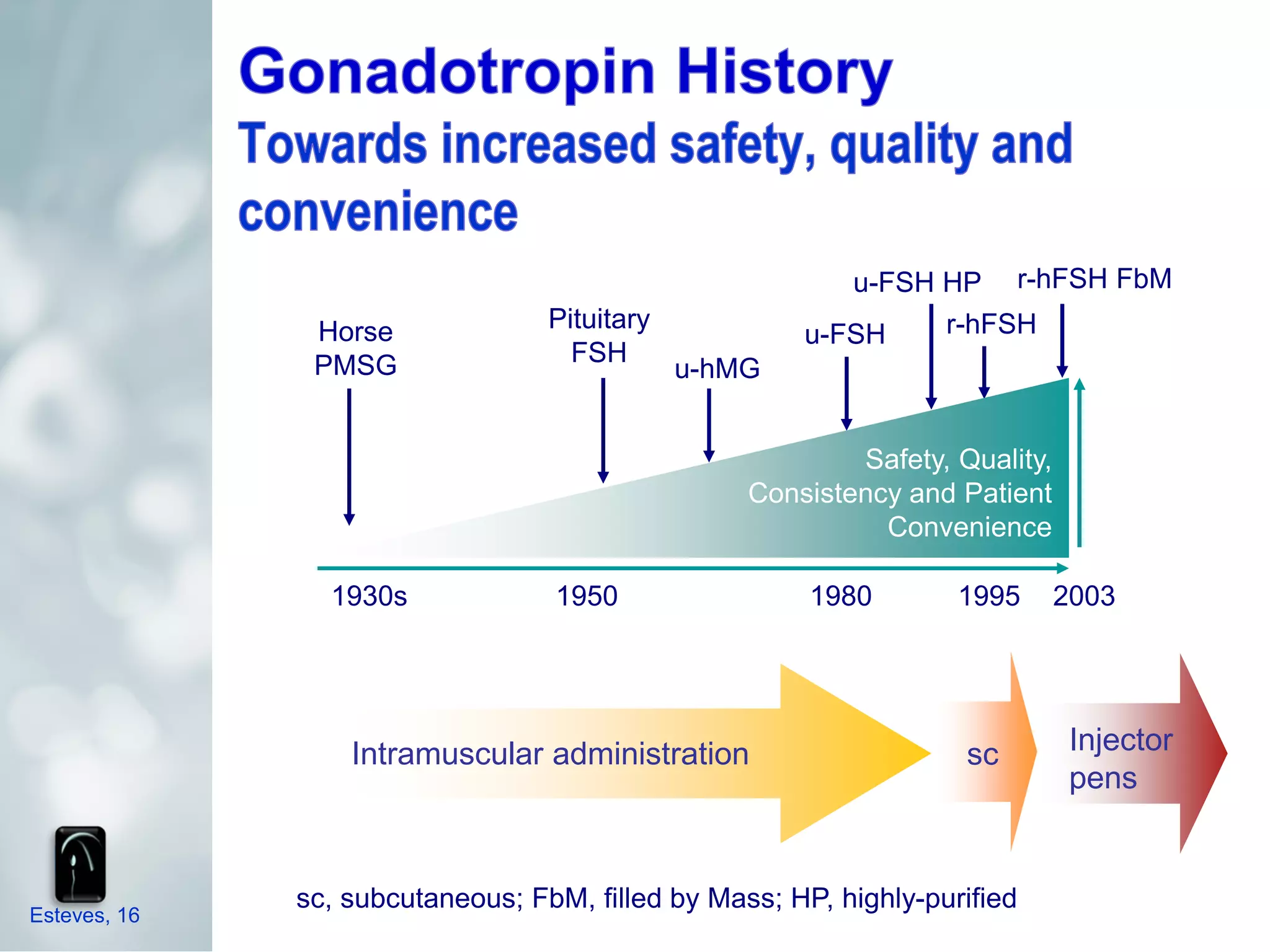
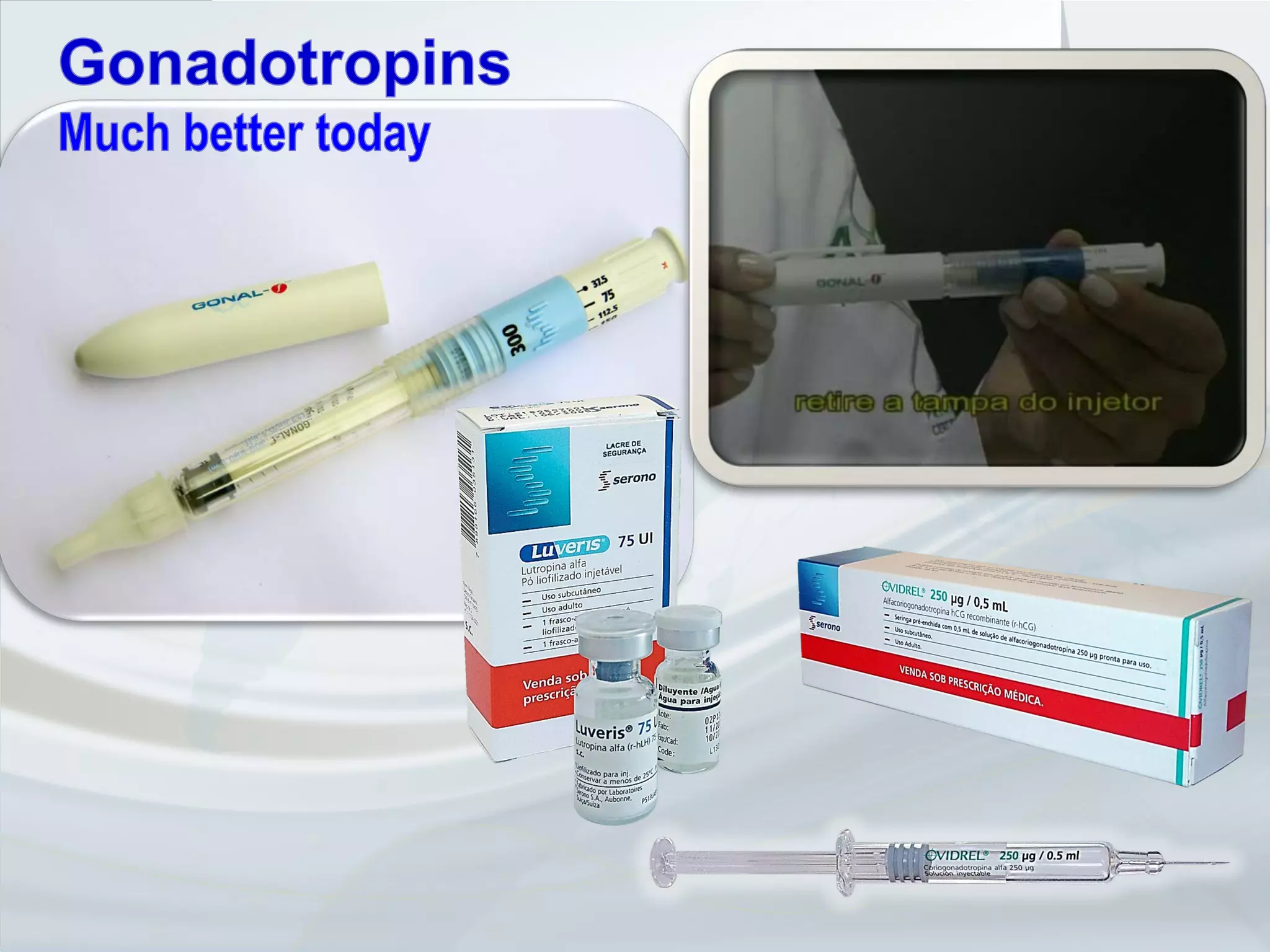
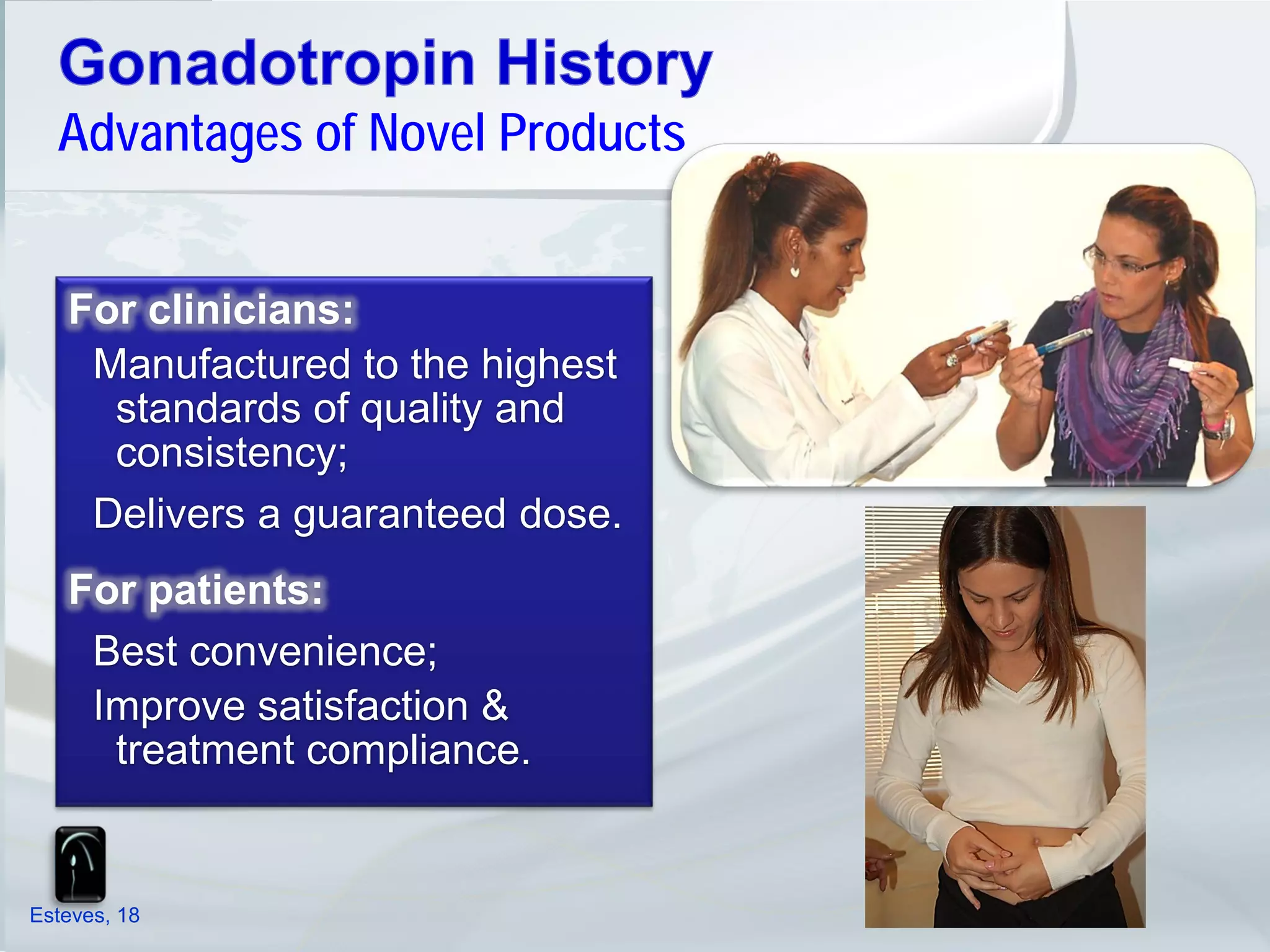
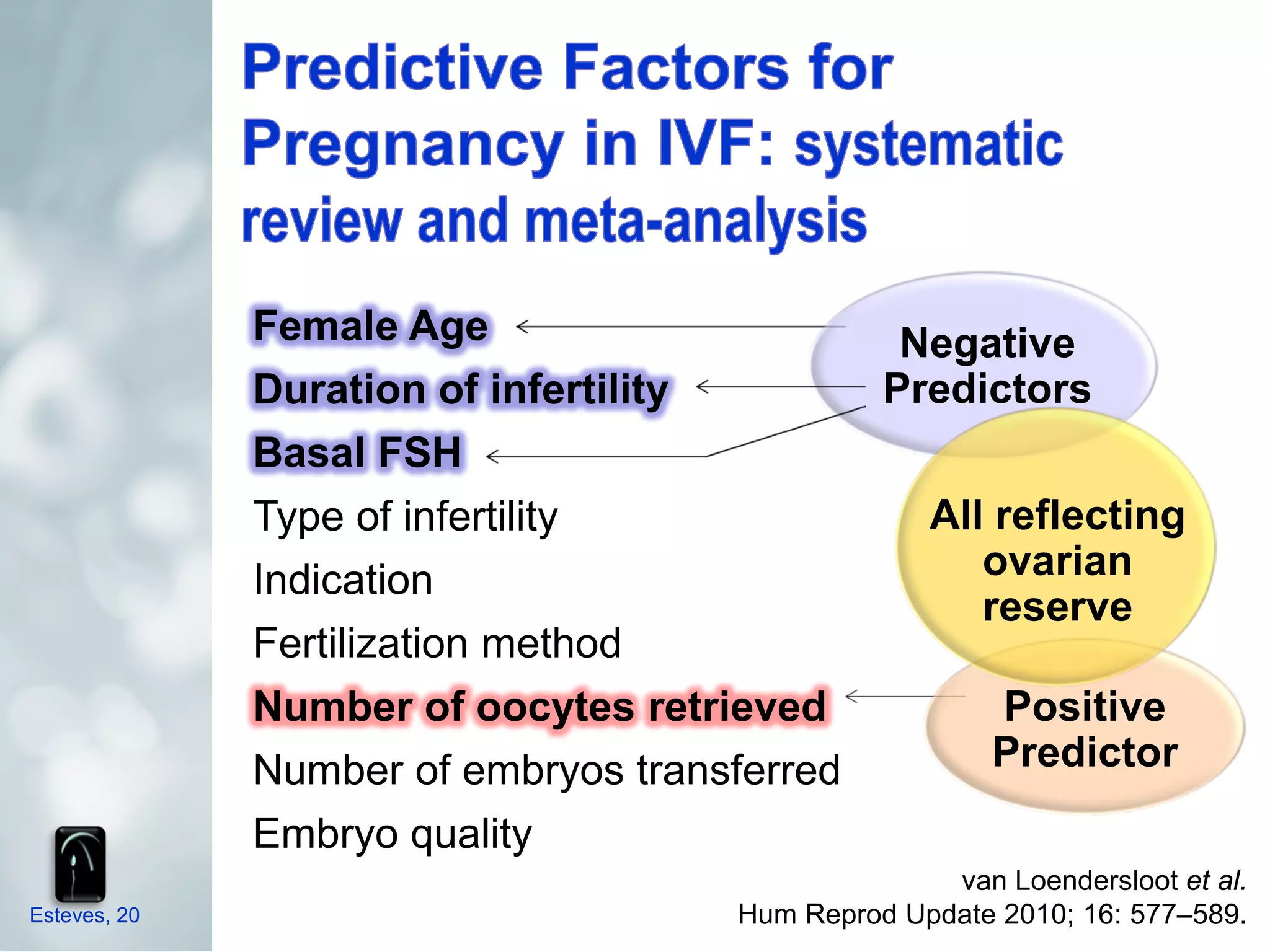
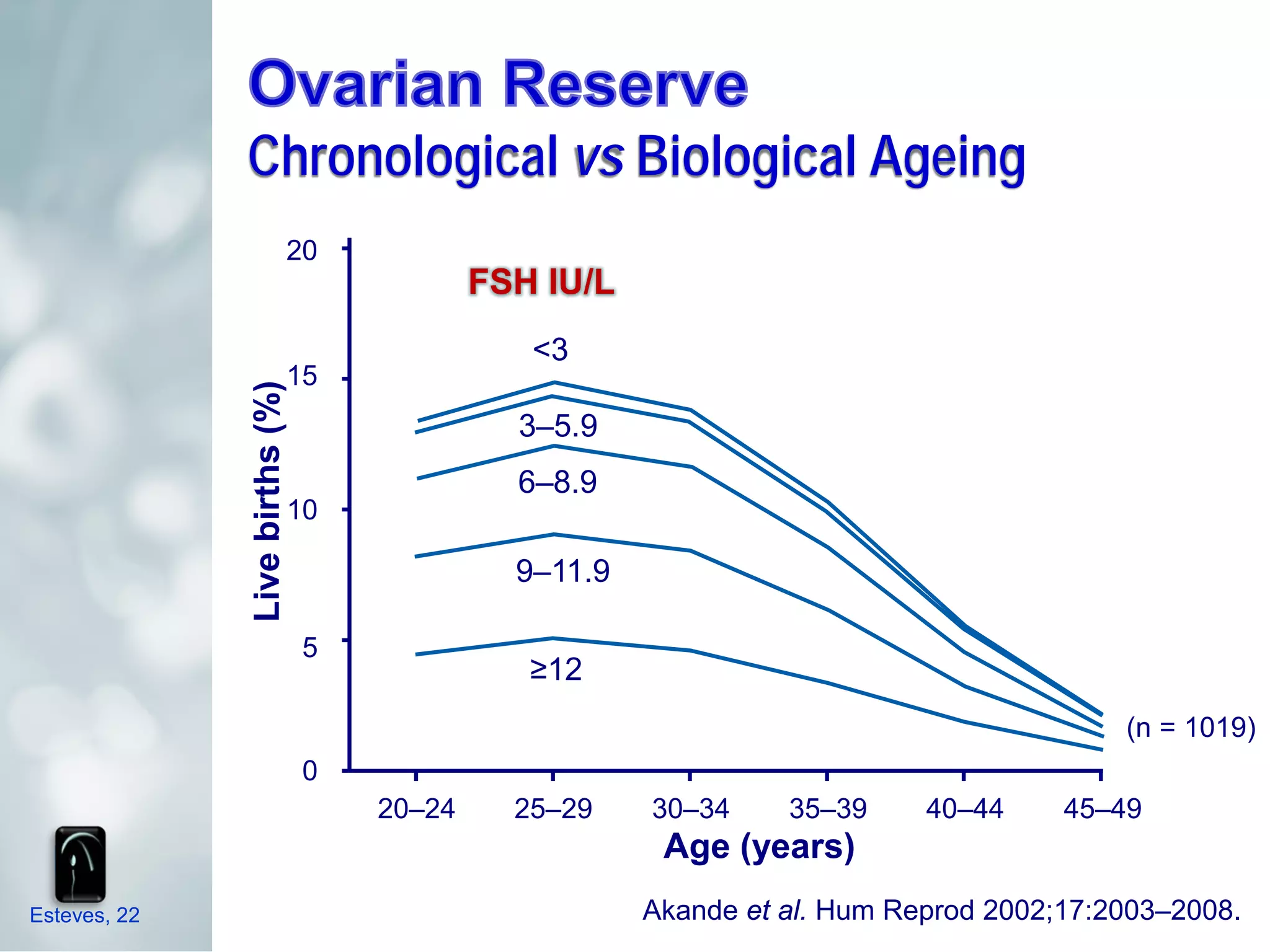
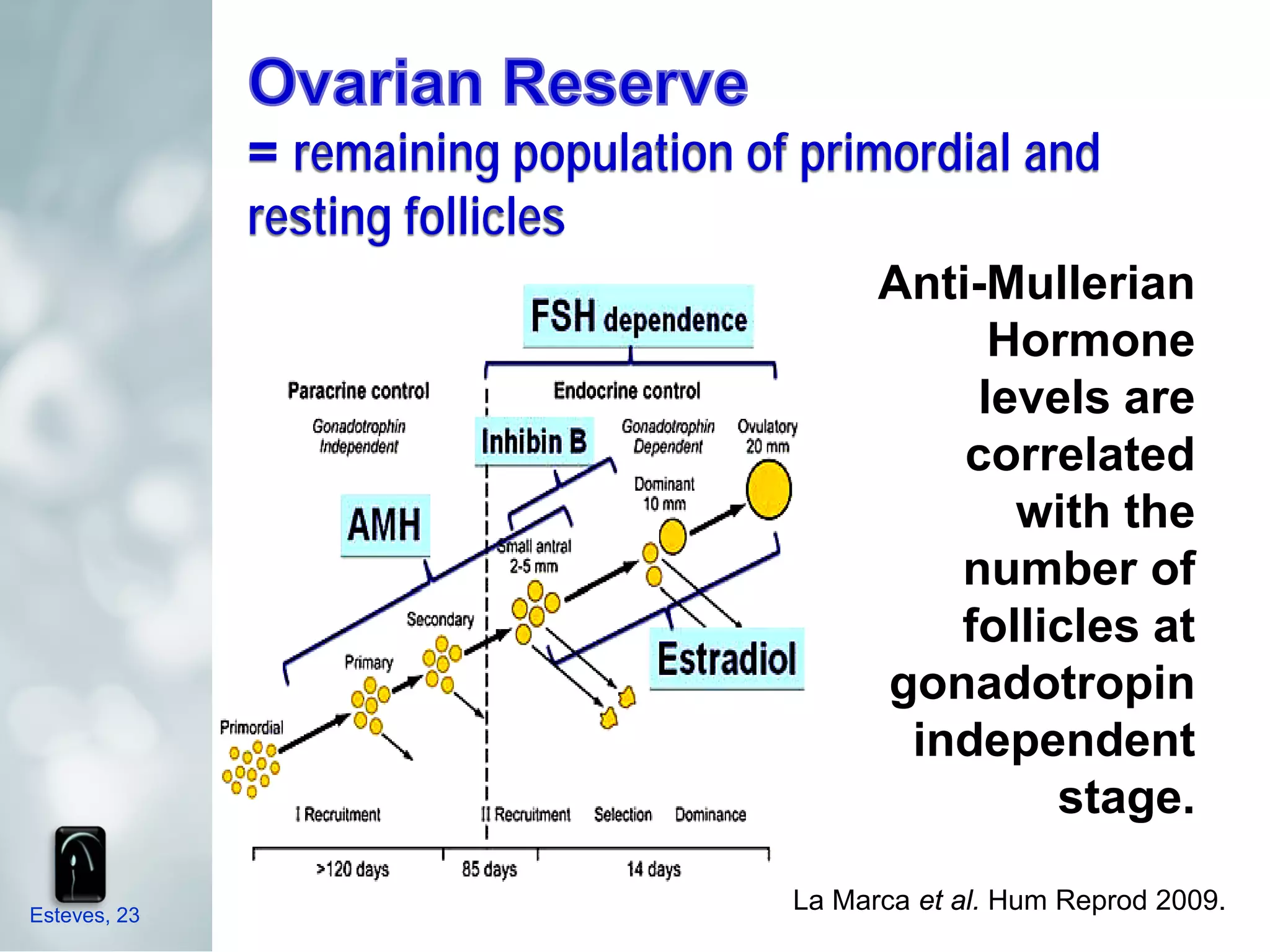
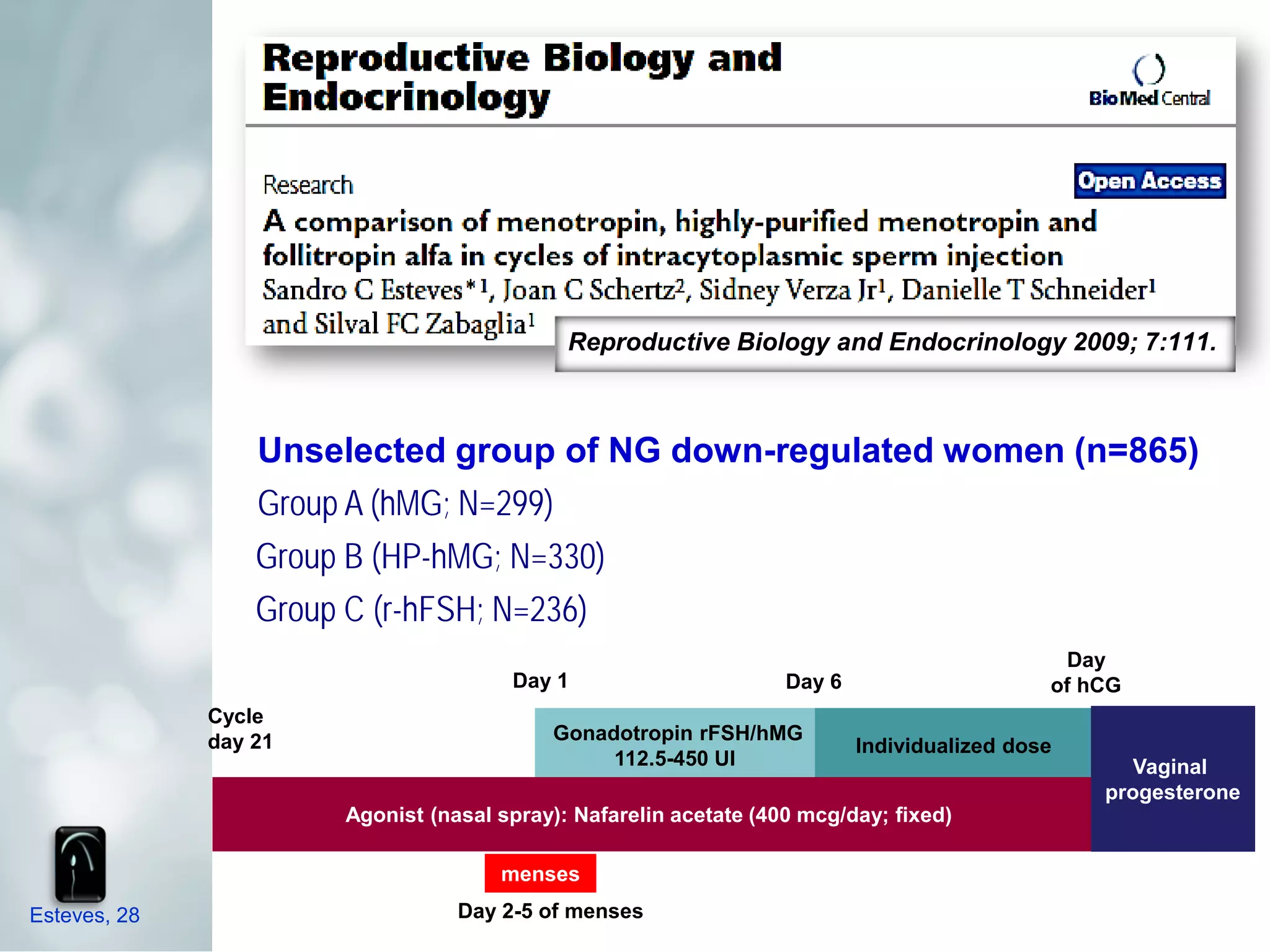
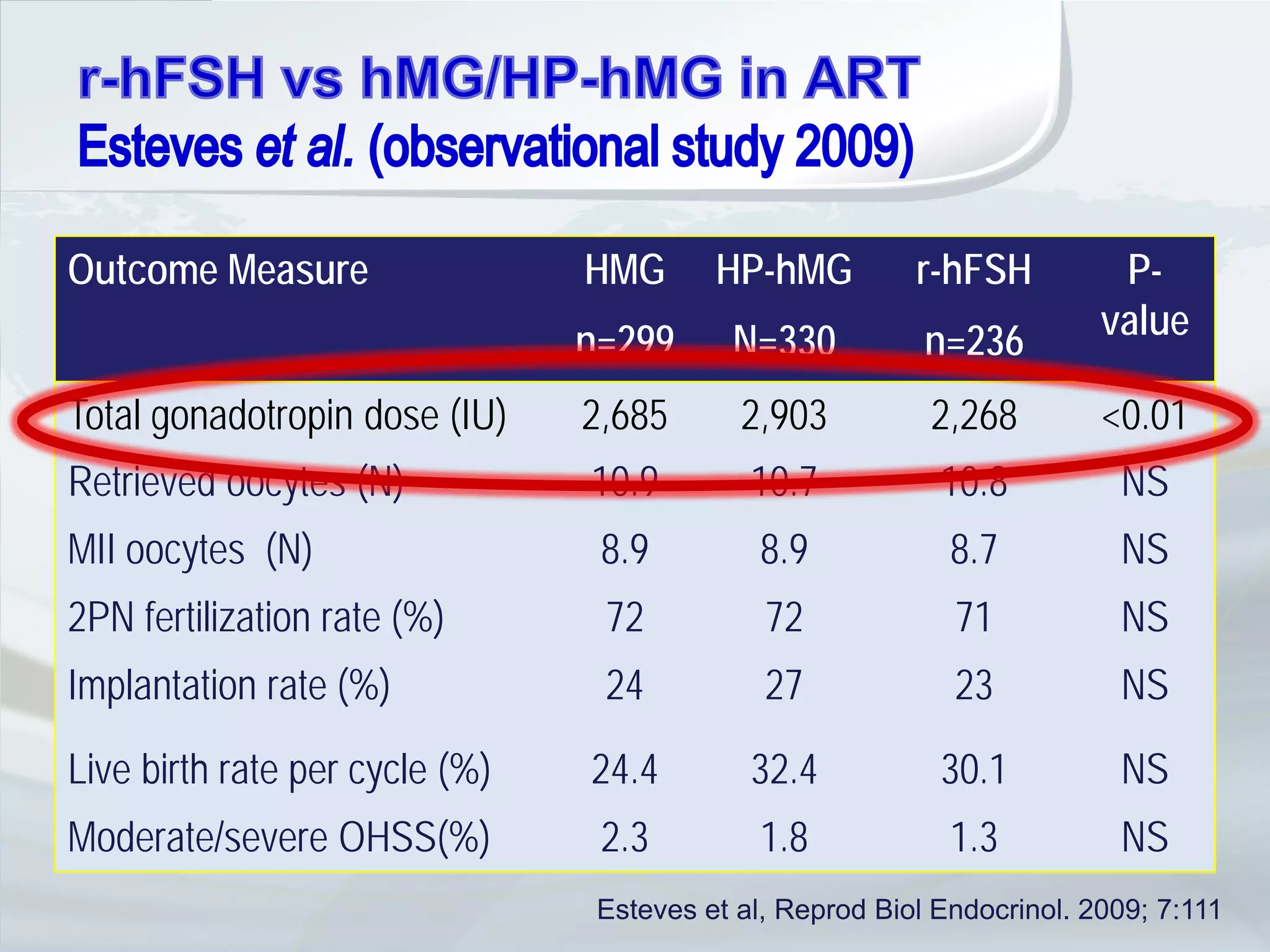
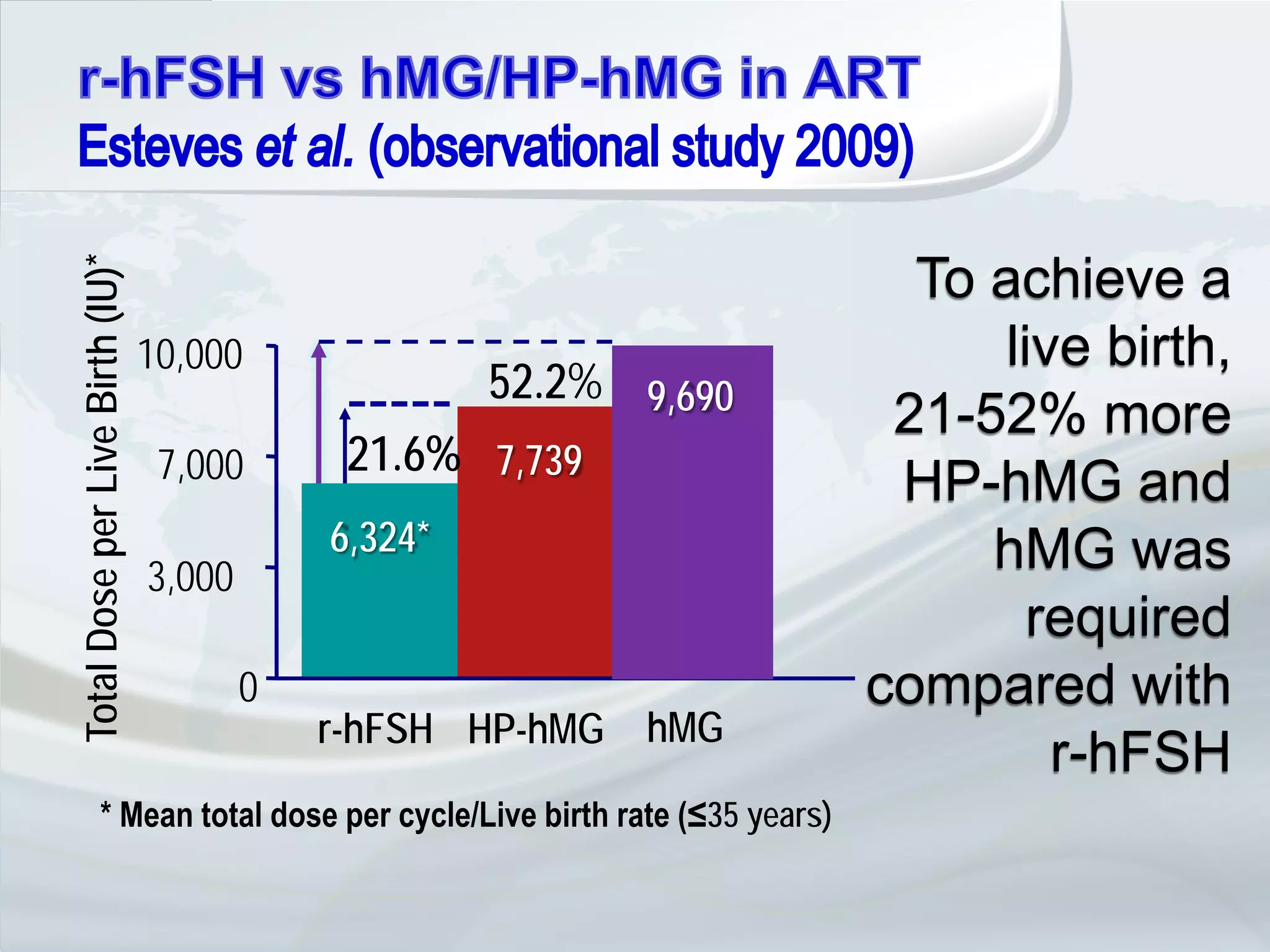
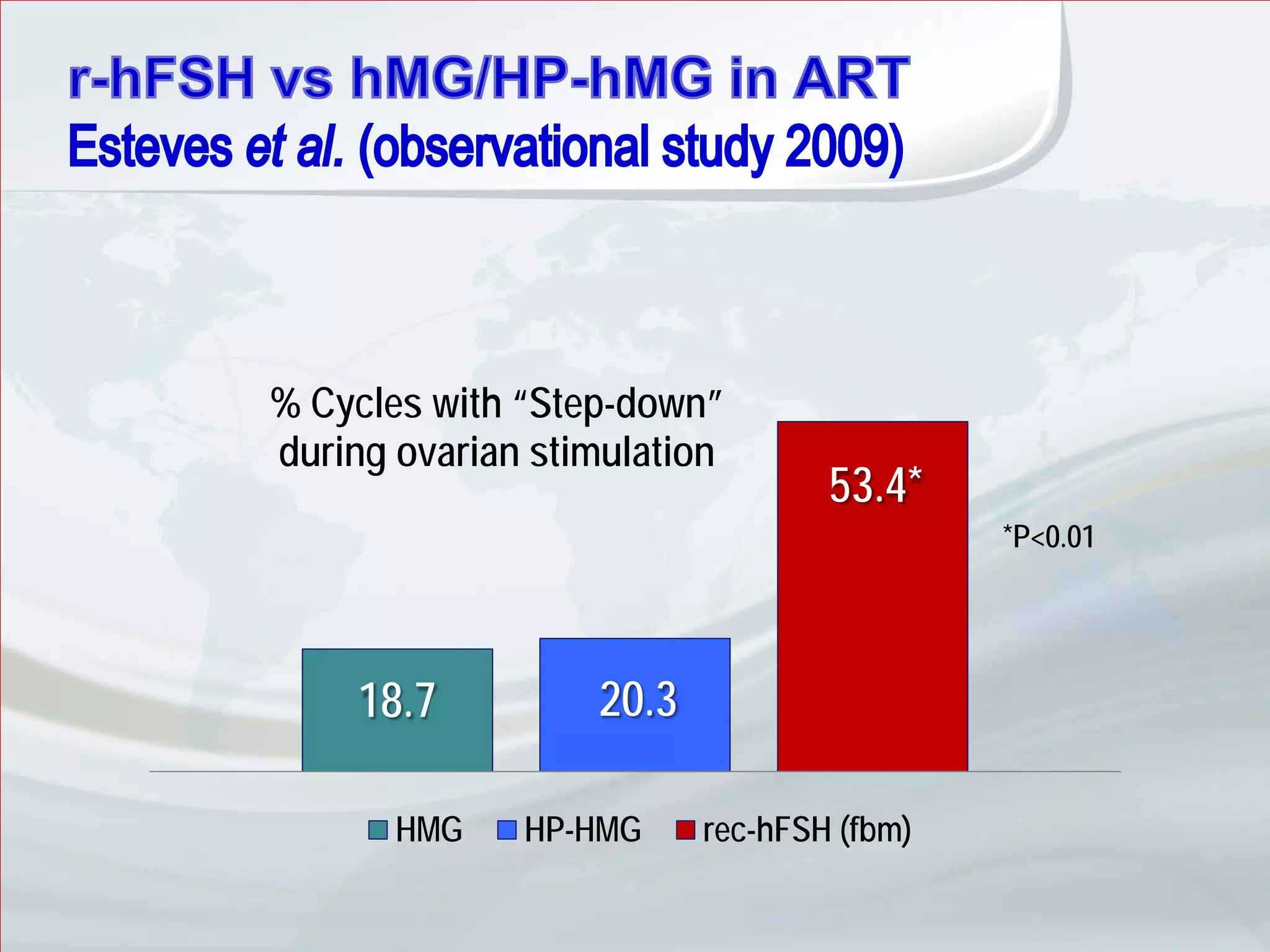
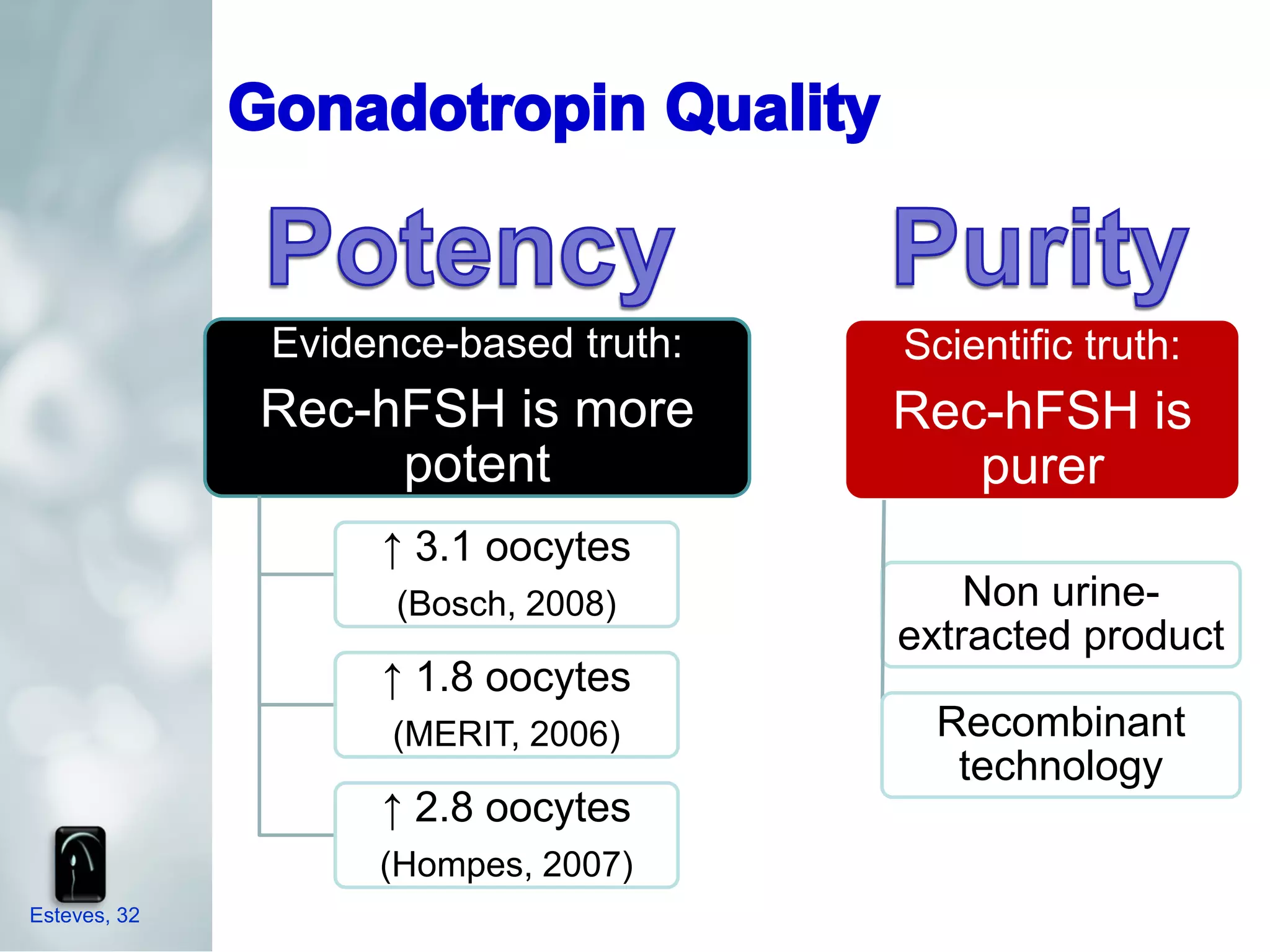
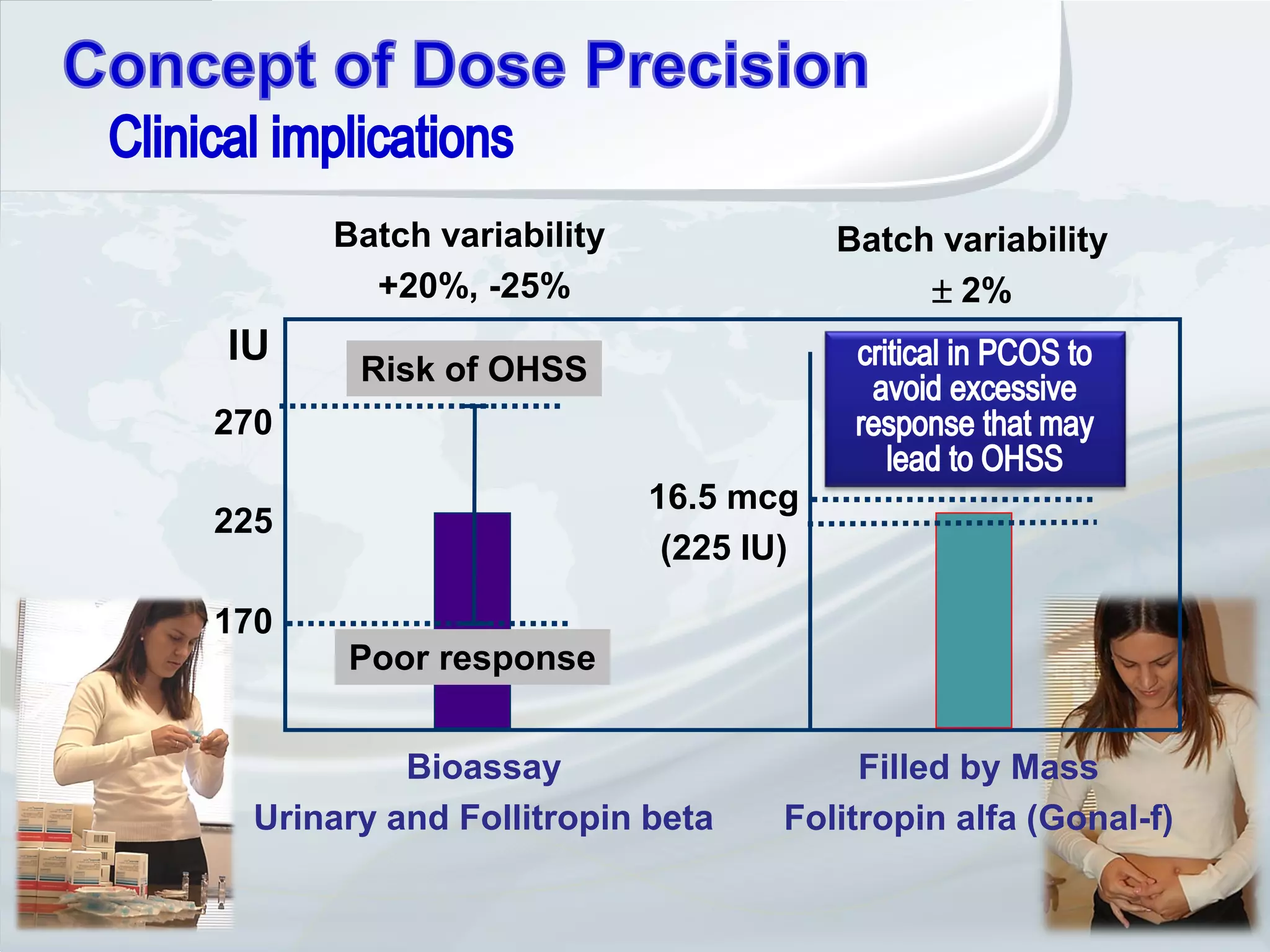
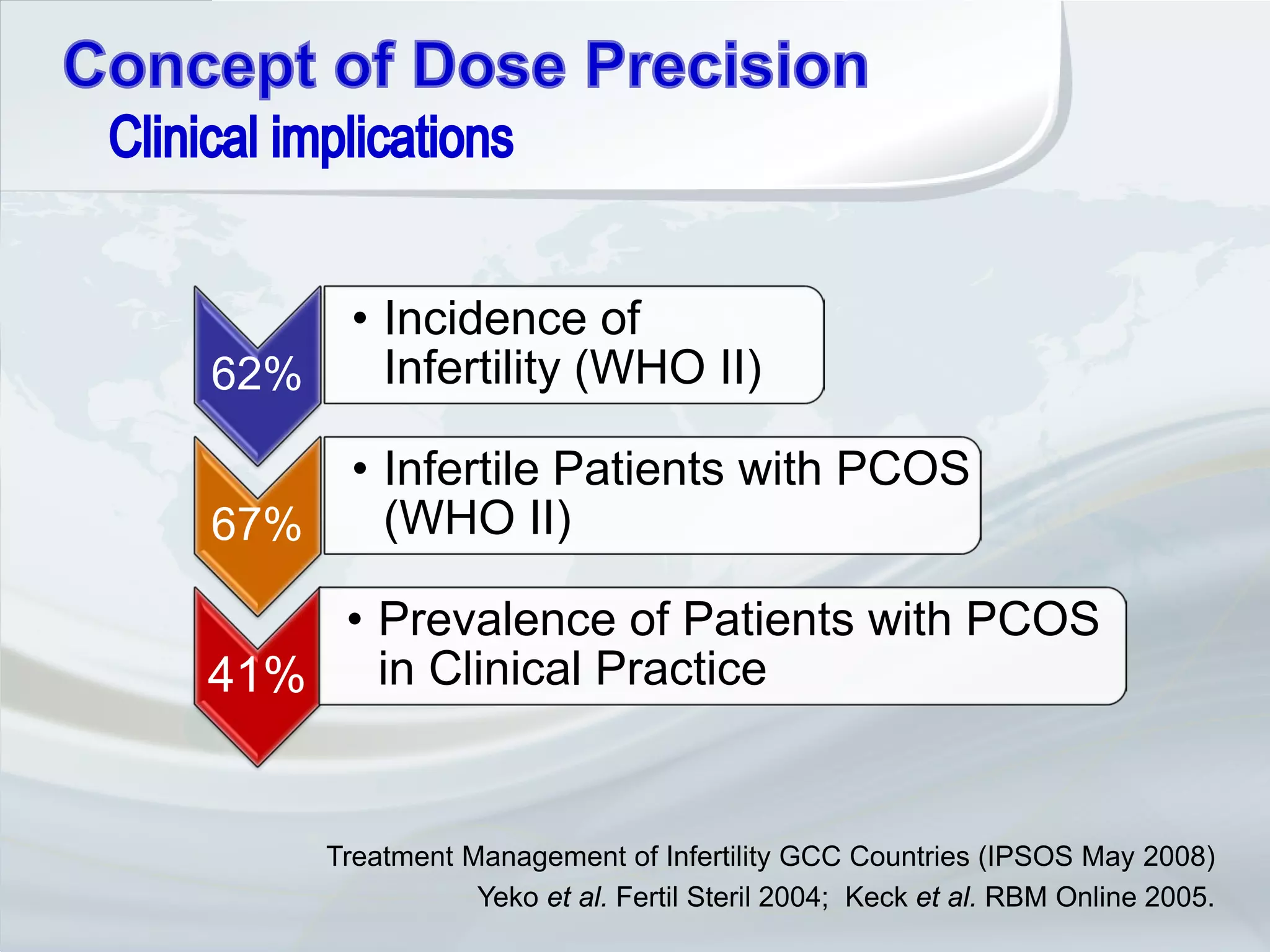

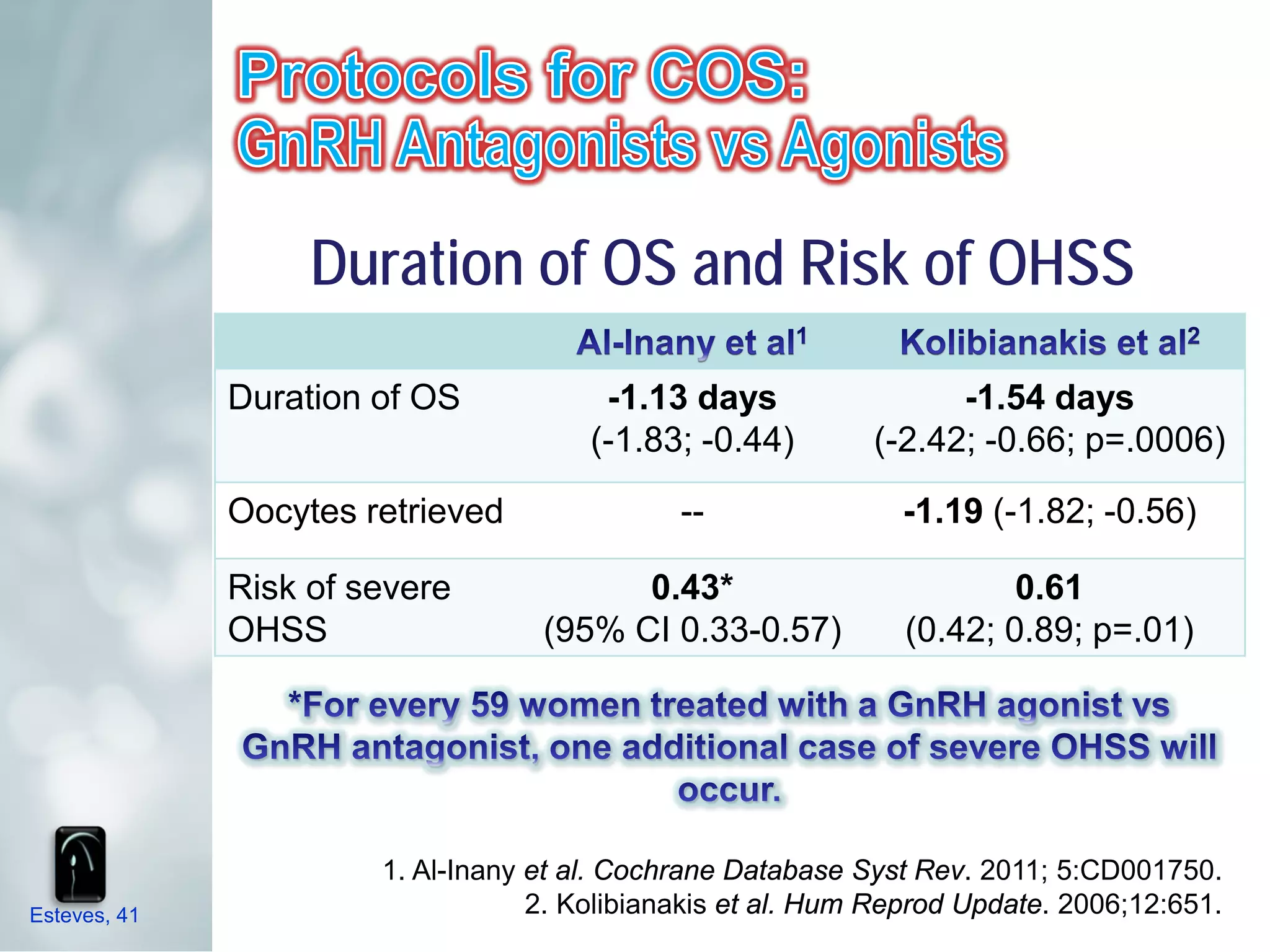
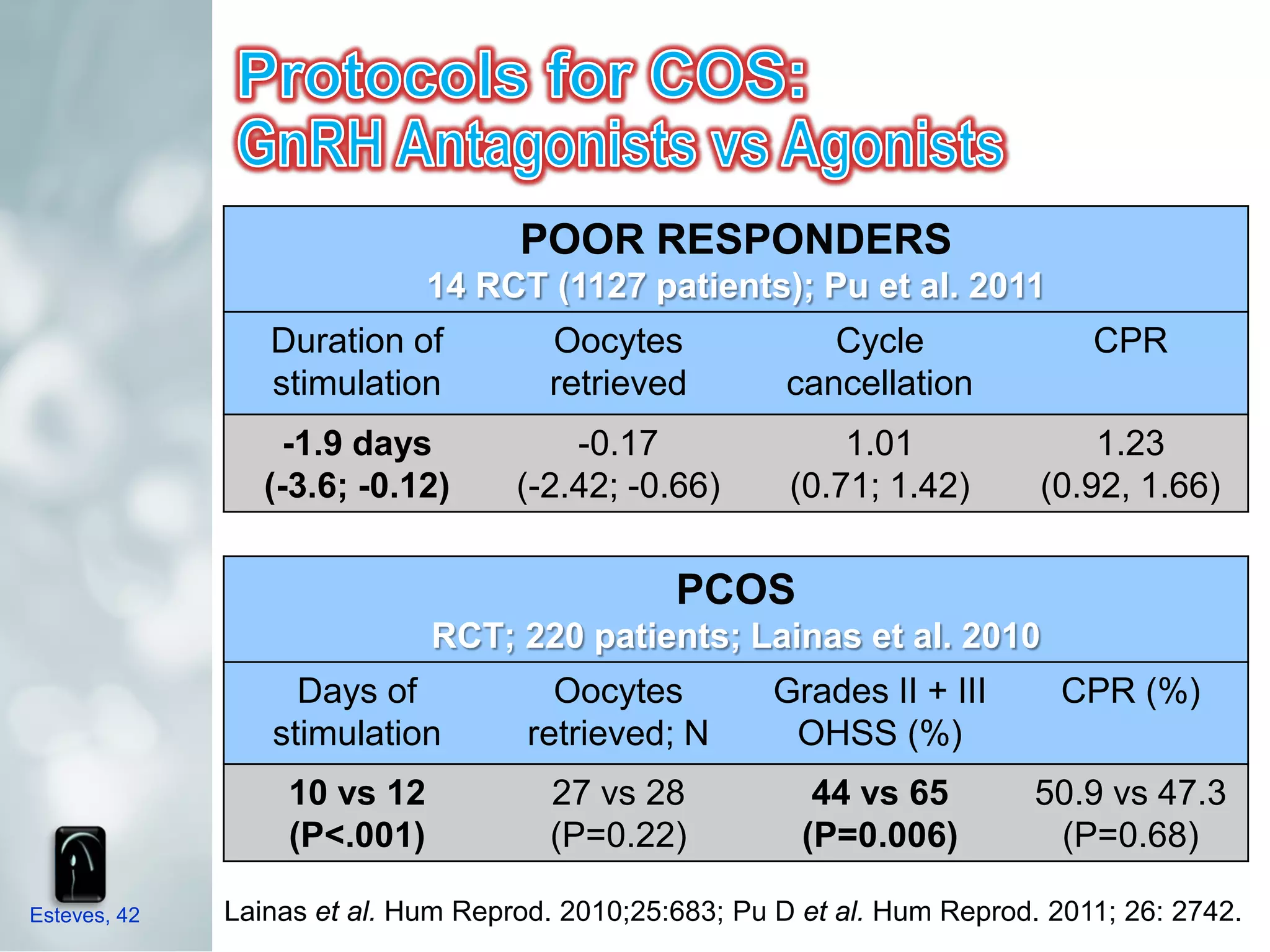
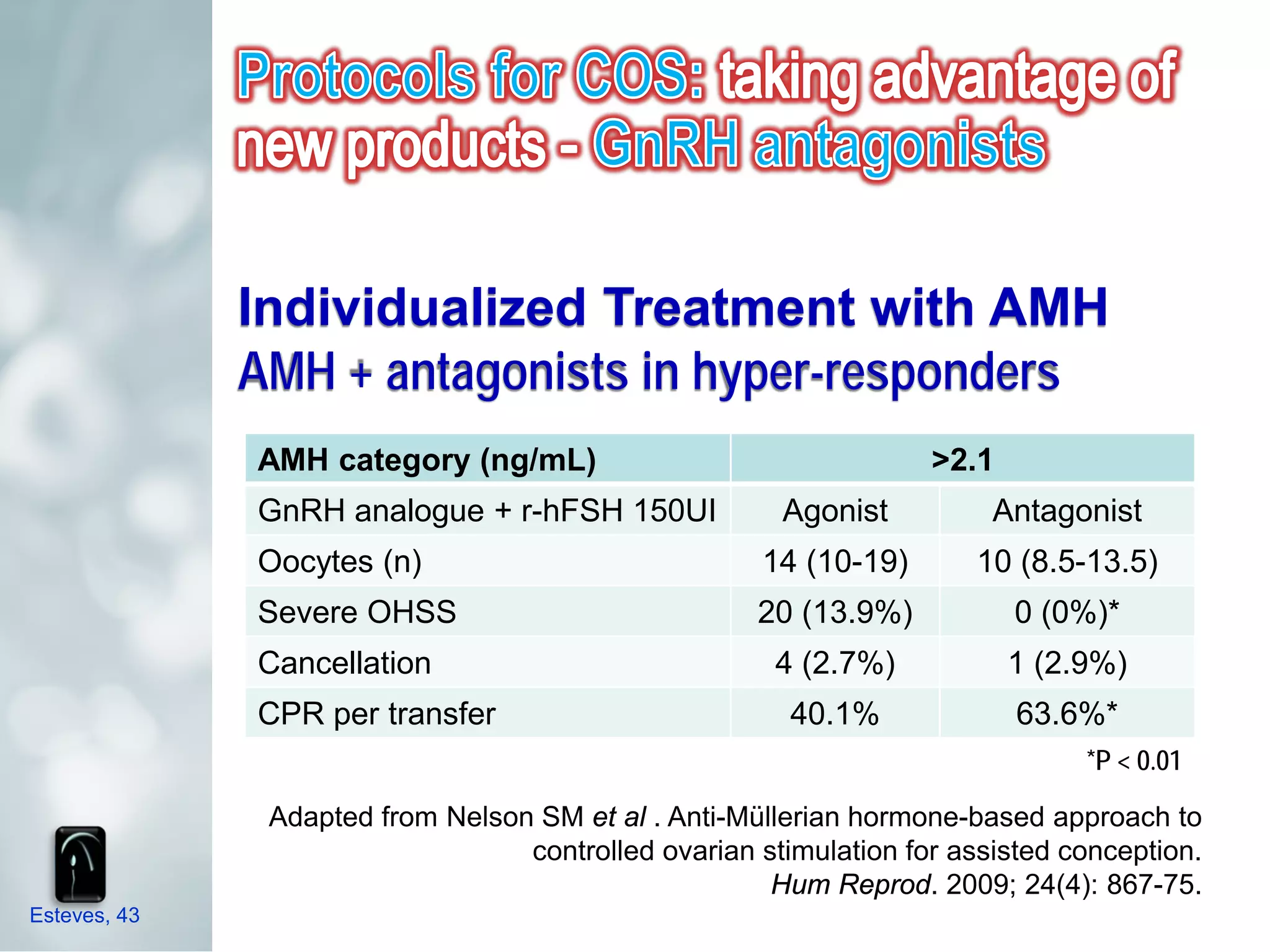
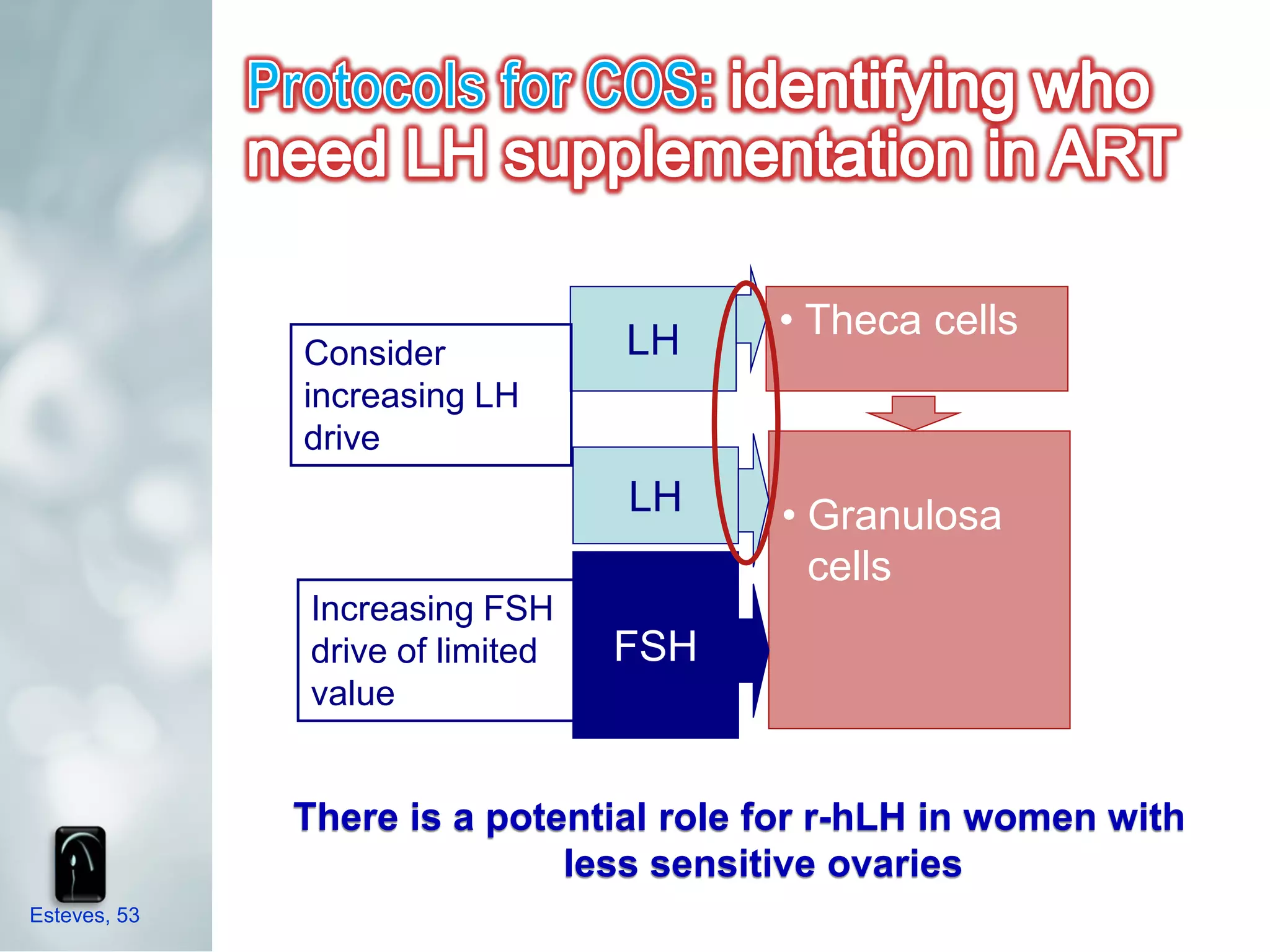
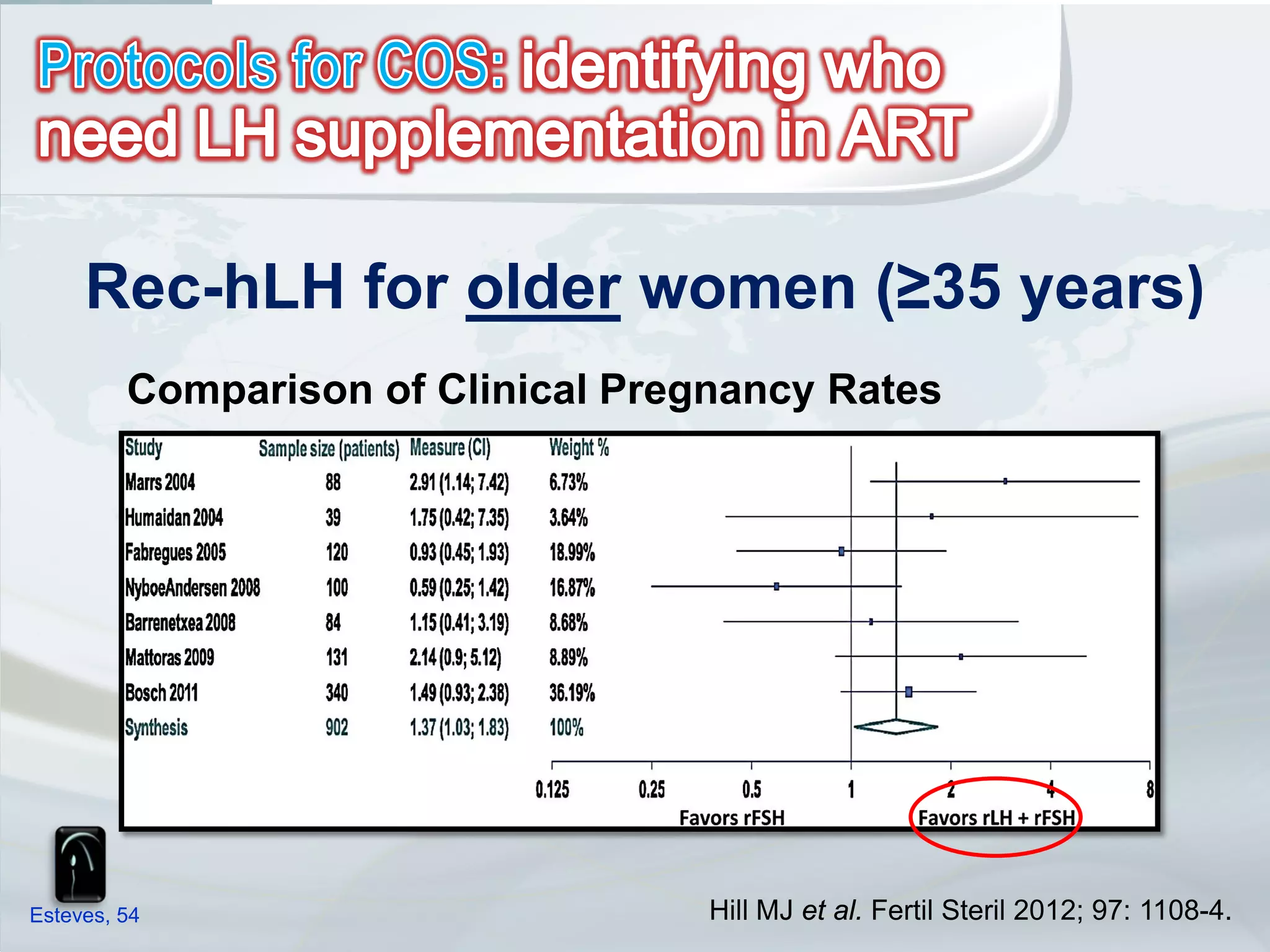
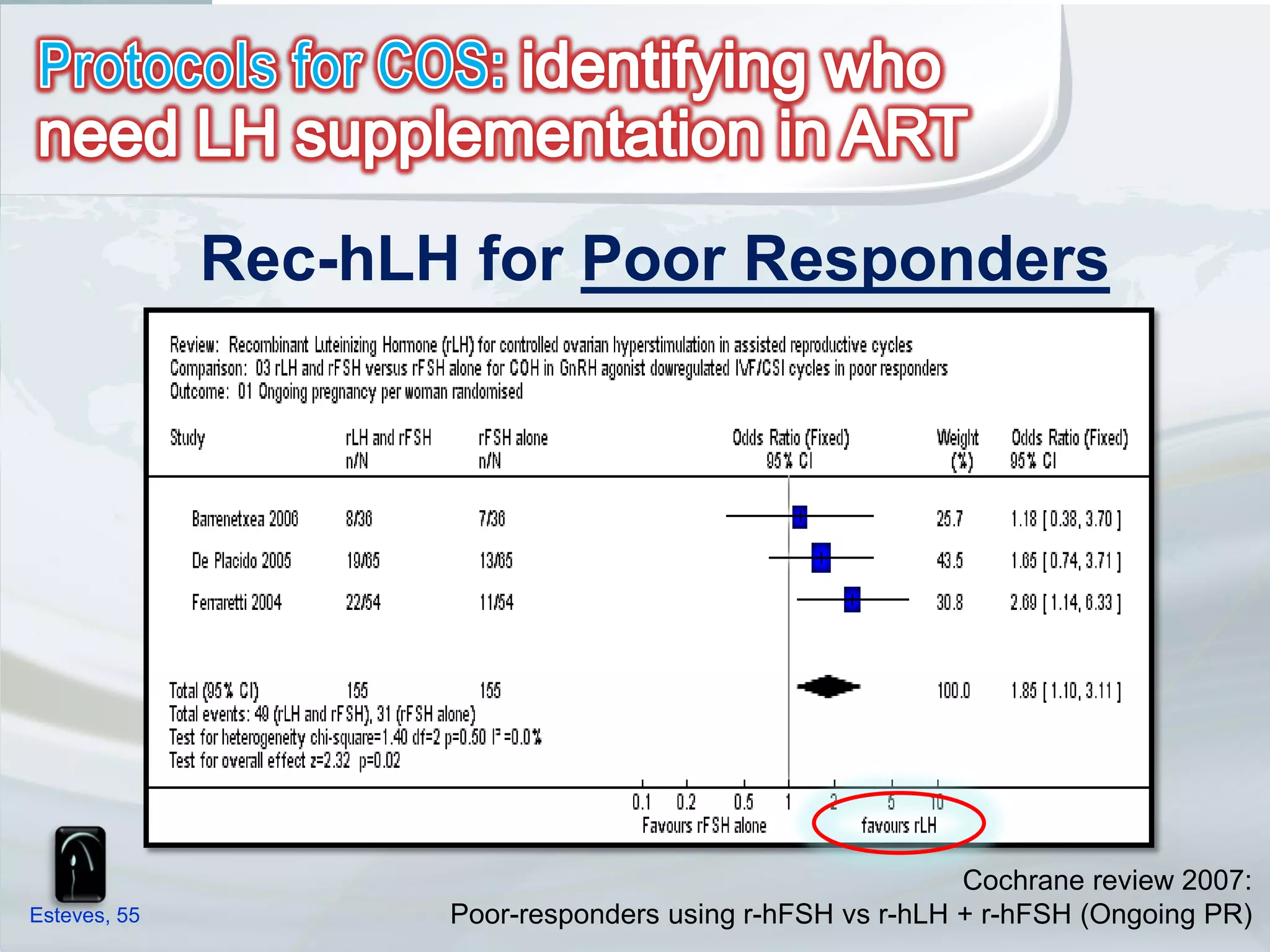
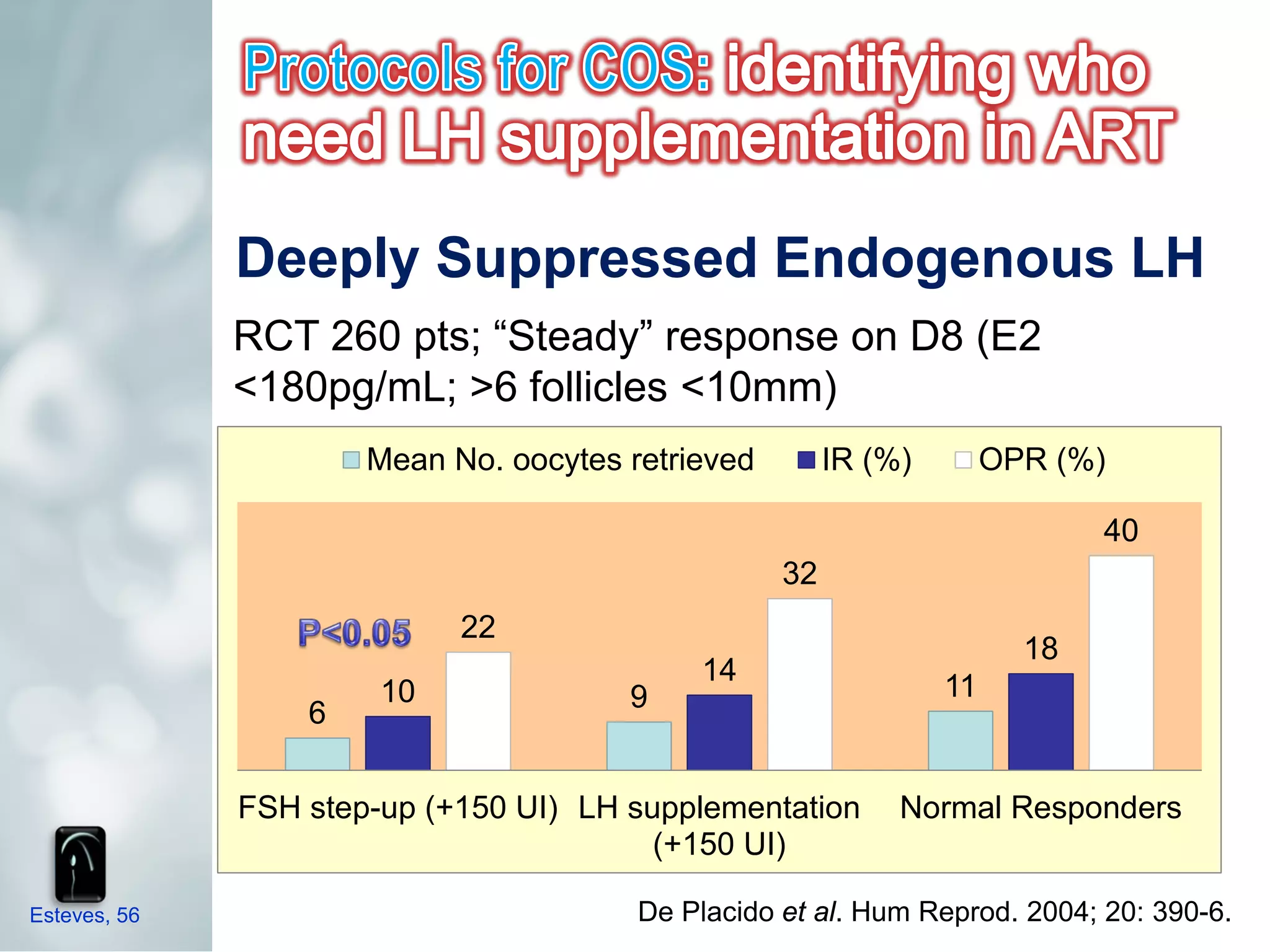
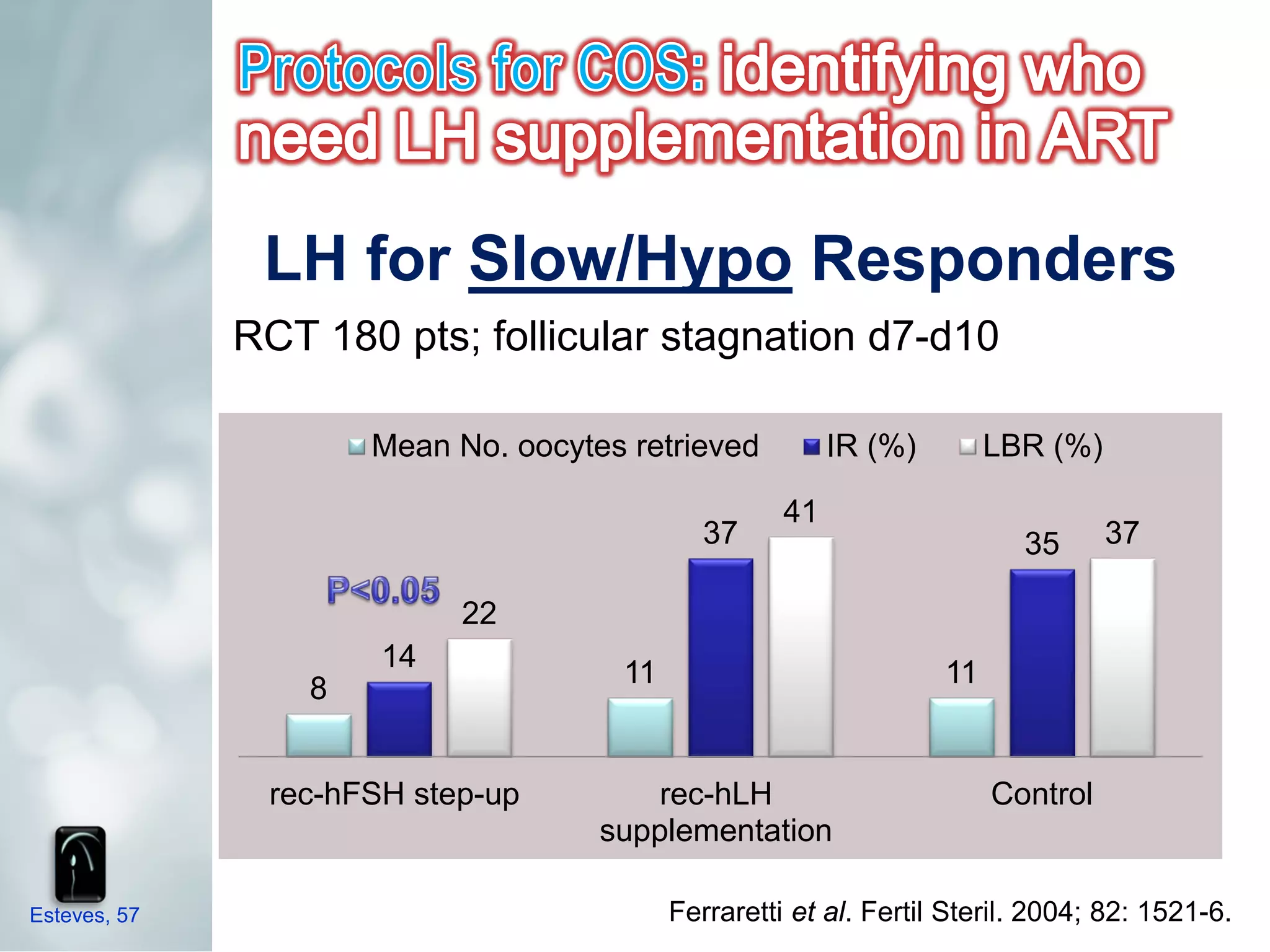
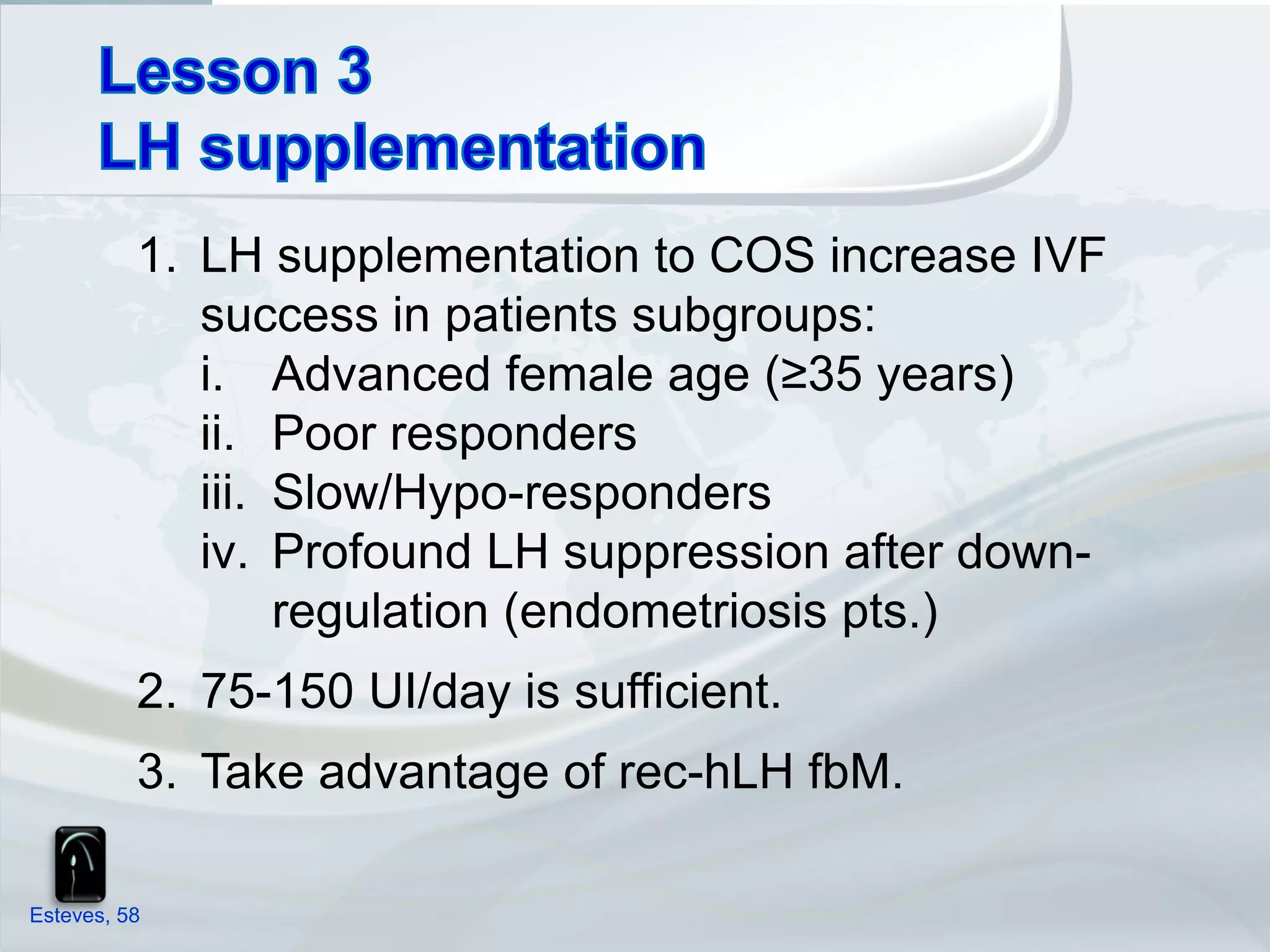
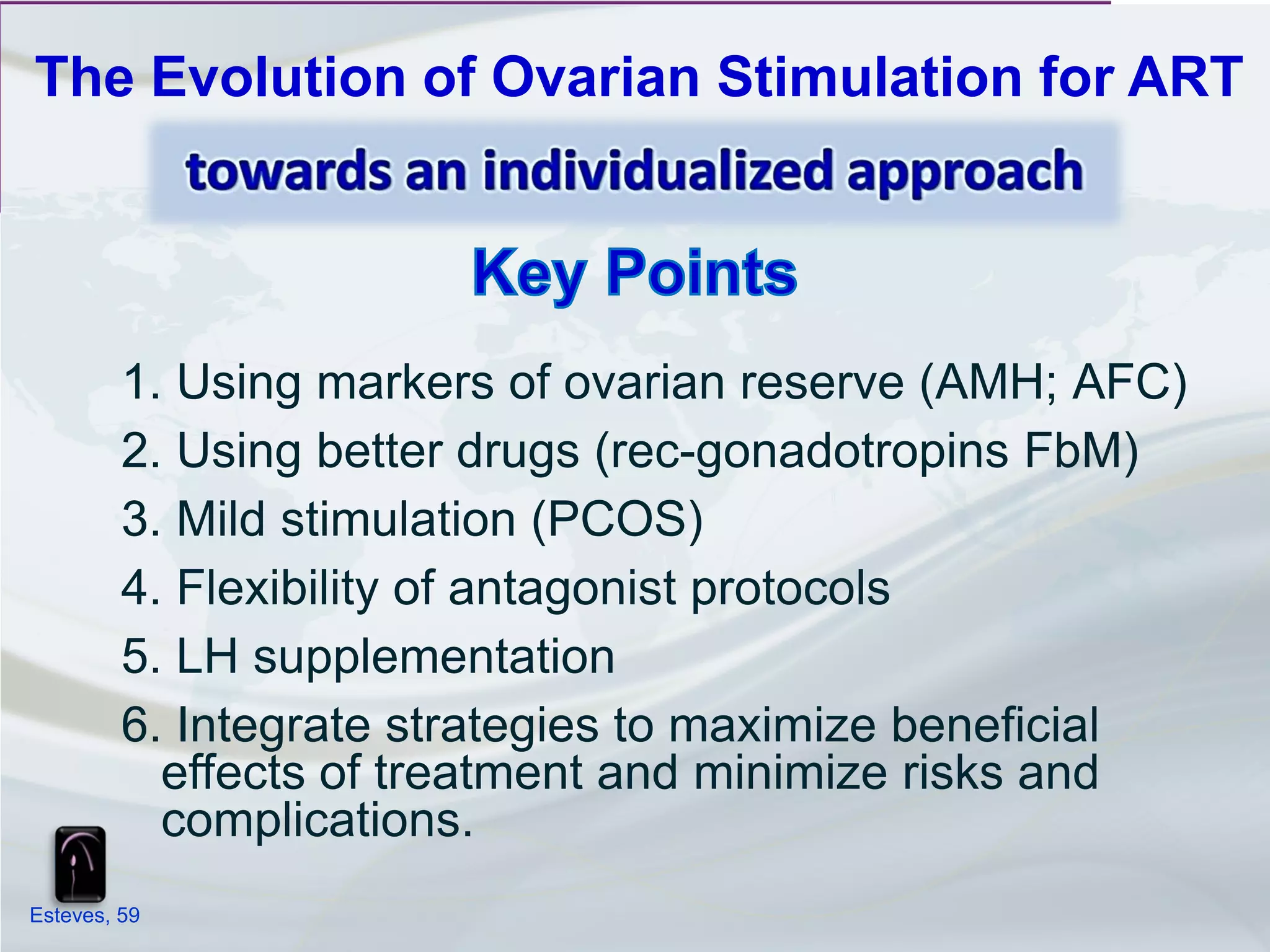


The presentation discusses the evolution of ovarian stimulation for assisted reproductive technology (ART). It begins with a historical perspective of gonadotropin development from urinary sources to recombinant products. It then examines primary factors affecting IVF success like age, ovarian reserve markers, and cause of infertility. The presentation concludes by exploring more individualized clinical strategies like tailoring gonadotropin doses, flexible GnRH antagonist protocols, and LH supplementation to improve IVF outcomes.























































































