- A 3 year 5 month old child presented with constipation since 6 months of age, which was diagnosed as functional constipation. Examination found a loaded colon on x-ray but no other abnormalities.
- Functional constipation is usually caused by painful bowel movements that cause voluntary withholding of stool. It is commonly treated with lifestyle changes like diet and behavior modifications, disimpaction if needed, and maintenance therapy using laxatives.
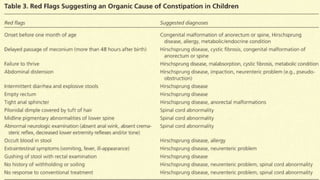
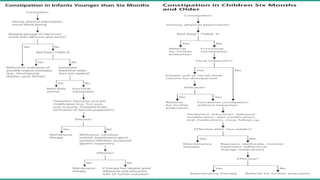
- Younger infants require more evaluation to rule out organic causes for constipation like Hirschsprung's disease. Older children may need further testing if constipation is intractable or there are red flags for underlying conditions.





























































































![Session 6 se and complications [repaired]](https://cdn.slidesharecdn.com/ss_thumbnails/session6seandcomplicationsrepaired-180404084057-thumbnail.jpg?width=640&height=640&fit=bounds)




















