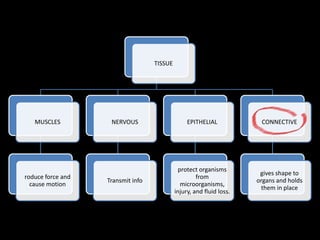
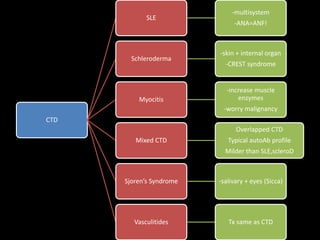
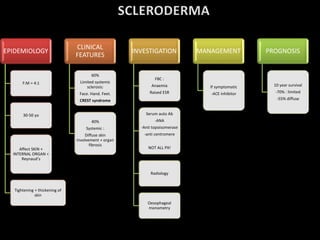
This document discusses several potential mechanisms that can lead to autoimmune diseases, including the release of sequestered antigens, molecular mimicry, superantigen infection, and mutations in genes regulating the immune response. It also provides an overview of different types of hypersensitivity reactions (types I-IV) and lists some common organ-specific and non-organ-specific autoimmune diseases. Finally, it briefly touches on epidemiology, etiology, clinical features, investigations, and management of systemic lupus erythematosus.
![• Injury antigen penetrate antigen activates T cells in
nodes T cells attach BOTH eyes
1. RELEASE OF SEQUESTERED
ANTIGEN
• Drugs : Hydralazine, penicillin2. ALTERATION OF SELF
• Antigen = mimic cardiac muscles
• Ie : RF, IE, post strep GN
3. MOLECULAR MIMICRY
• Uncontrollable massive T-helper cells expansion
• Loss of specificity [defense of antigen]
4. SUPERANTIGEN INFECTION
• Presence of signal 2 [x peripheral T-cell tolerance]
• Signal 2 : infection activation
5. INFECTION OF APC
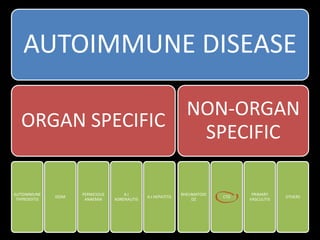
• ALPS
• fas/fas ligand mut no apoptosis of lymphocytes ON!
6. MUTATION IN GENES
REGULATING IMMUNE RESPONSE
‘Leaky ‘
tolerance
Autoimmune
reactivity
Autoimmune
dz](https://image.slidesharecdn.com/ctd-170622125340/85/Connective-tissue-disease-1-320.jpg)
![• Antigen + antibody
• Antibody agglutinate to form button
• PROB : if [Ab] highfalse –ve,
therefore try at different [ ] dilute
AGGLUTINATION ASSAYS
INDIRECT
IMMUNOFLOURESCENCE
ELISA](https://image.slidesharecdn.com/ctd-170622125340/85/Connective-tissue-disease-2-320.jpg)
![TYPE II HS
[Ab mediated
cytotoxicity]
MECHANISM LAB TEST
TYPE III HS
[immune complex
deposition]
MECHANISM LAB TEST
TYPE IV HS
[delayed HS]](https://image.slidesharecdn.com/ctd-170622125340/85/Connective-tissue-disease-3-320.jpg)
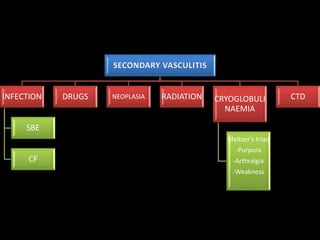
![SPECTRUM
APS
-thrombosis
Latent lupus
Neonatal
lupus
End stage
lupus
Drug-induced
lupus
EPIDEMIOLOGY
F:M = 9:1
Dz of young
women [20-
30 yo]
Black>white
Genetics ass.
C4A null alleles
AETIOLOGY
Unknown but
multifactoral
Genetics
-If
HLAB8,DR2,D
R3 +ve
10% risk
immunologic
al
drugs
Infection :
EBV
Sex hormones
CRITERIA
A RASH POINTS
AN MD
-Malar rash
-Discoid rash
-
photosensitivity
-oral/nasophra
Ulcer
-arthritis
-serositis
-renal d/o
-neuro d/o
-haematolgic
-immuno. d/o
ANA test +ve
INVESTIGATION
FBC- anaemia
High ESR, N
CRP
Serum
autoAb:
-ANA
-anti-dsDNA
-RF
Anti
cardiolipin
[APS]
Histology
Urine cast :
RBC, Protien
TREATMENT
Gluco
corticoid
NSAID
Immuno
supressant
-anti malaria
Remitting relapse!
Different complaint. Urm...
UV light](https://image.slidesharecdn.com/ctd-170622125340/85/Connective-tissue-disease-7-320.jpg)
![DEFINITION +
EPI
Inflam and
necrosis of skeletal
muscle fibre + rash
Peak : childhood +
5/6th decade
CLINICAL
FEATURES
Photosensitive
rash
SKIN CHANGES :
-heliotrope
periorbital rash
-gottren’s papule
-erythema on
nailbed
Symmetrical
progressive muscle
weakness
INVESTIGATION
Muscle test/exam
wasting
Muscle enzymes
[CPK,LDH,AST,
aldolase]
EMG
Muscle biopsy
Lymphatic
infiltrate +
necrosis
ANF / others
MANAGEMENT
Oral prednisolone
Immunosupressive
therapy
Screen for
malignancy
PROGNOSIS
50% affected
children die within
2 years
Adult better
prognosis
15-30% elderly px
ass. cancer
Inclusion body myositis?](https://image.slidesharecdn.com/ctd-170622125340/85/Connective-tissue-disease-9-320.jpg)
![DEFINITION
Inflammation
within the
BV,disrupting the
internal elastic
lamina
May involve :
-many/single organ
-different vessels’
size + type
CLASSIFICATION
CAUSES :
-PRIMARY
-SECONDARY
VESSELS’ SIZE:
-LARGE
-MEDIUM
-SMALL
DIAGNOSIS
Serology : ANCA
Biopsy
-affected organ/
blind
-granulomata?
Angiography : large
V
TREATMENT
Large : steroids
Medium/Small :
steroids + IV
cyclophosphamides
Immunosuppressive
: azathioprine
[steroid sparing tx]
Vasculitis?](https://image.slidesharecdn.com/ctd-170622125340/85/Connective-tissue-disease-10-320.jpg)