Downloaded 154 times
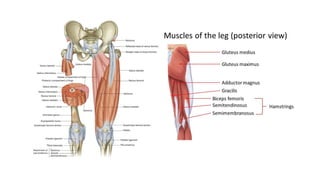

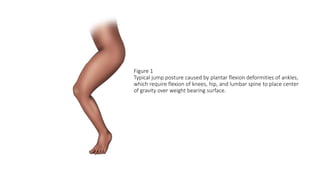

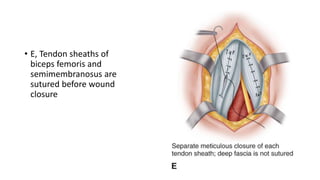







This document provides an overview of knee deformities in cerebral palsy and treatments for flexion deformity. It discusses how the hip and knee are related through connecting muscles. Flexion deformity is the most common knee issue and can be caused by tight hamstrings, weak quads, or other factors. Evaluation involves assessing various muscles for spasticity and strength. Common surgical techniques discussed include fractional lengthening of the hamstring tendons and combined hamstring lengthening with posterior capsule release. Distal femoral extension osteotomy with patellar tendon advancement is also summarized.








































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


