Downloaded 25 times


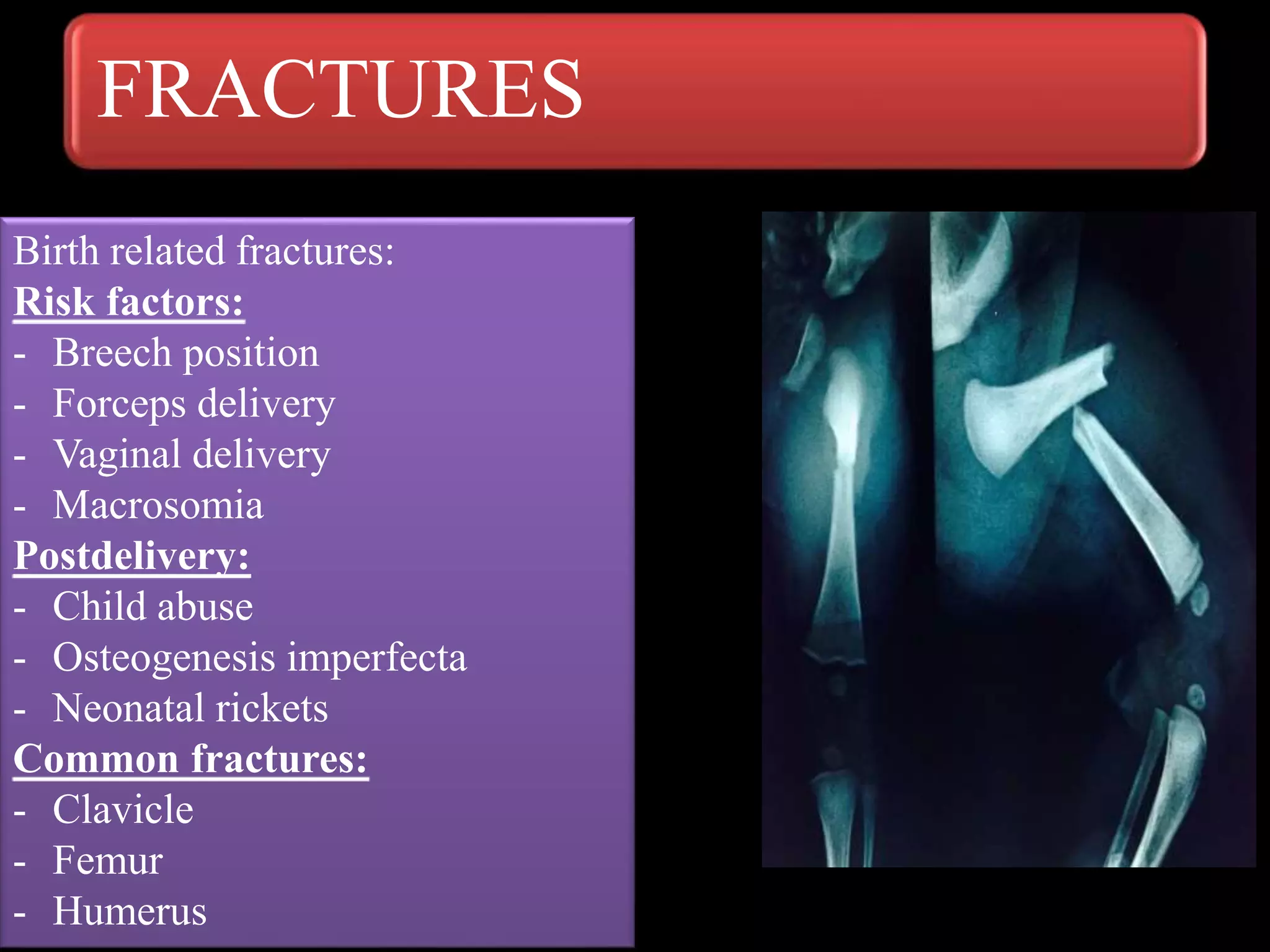

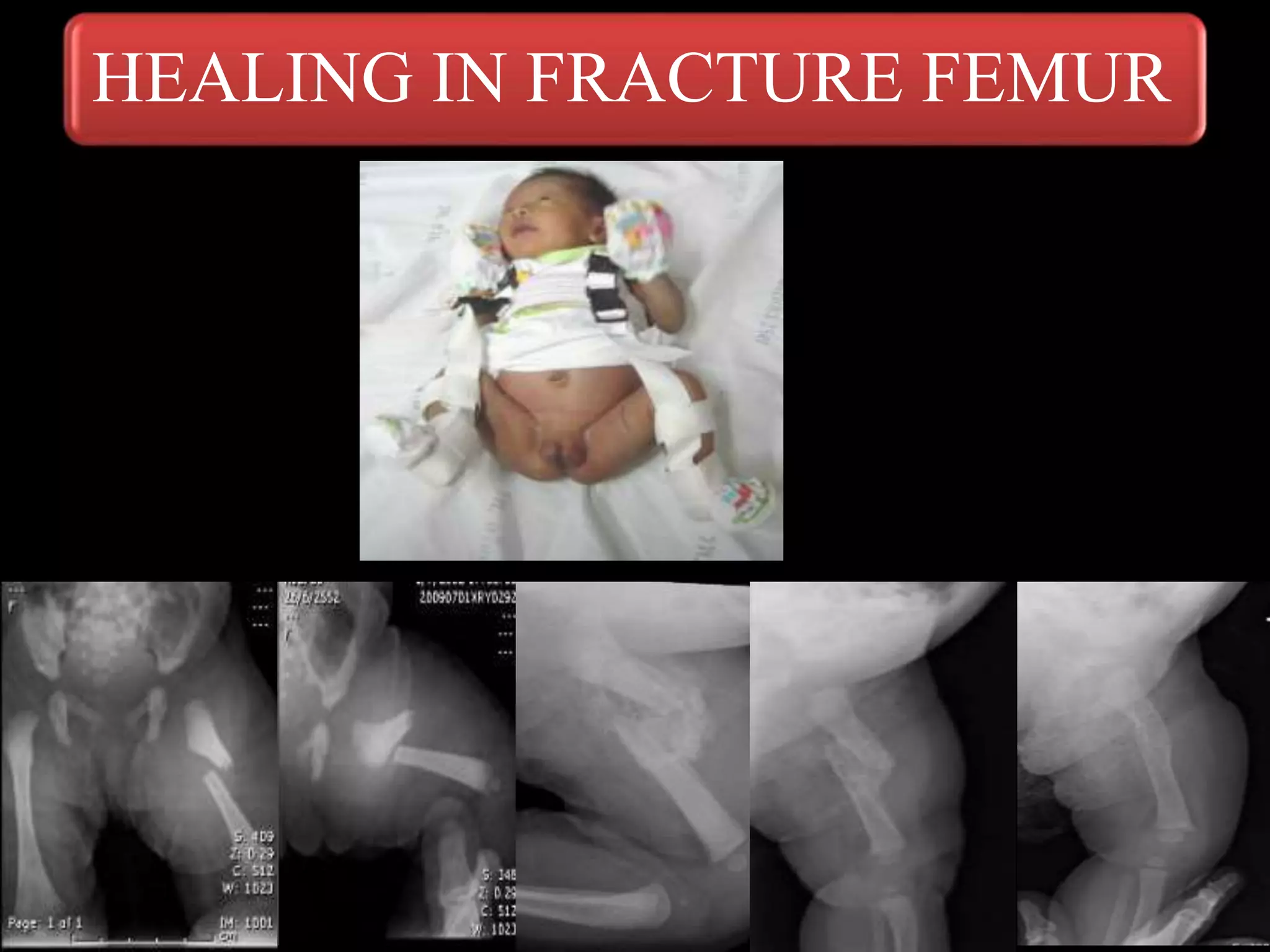
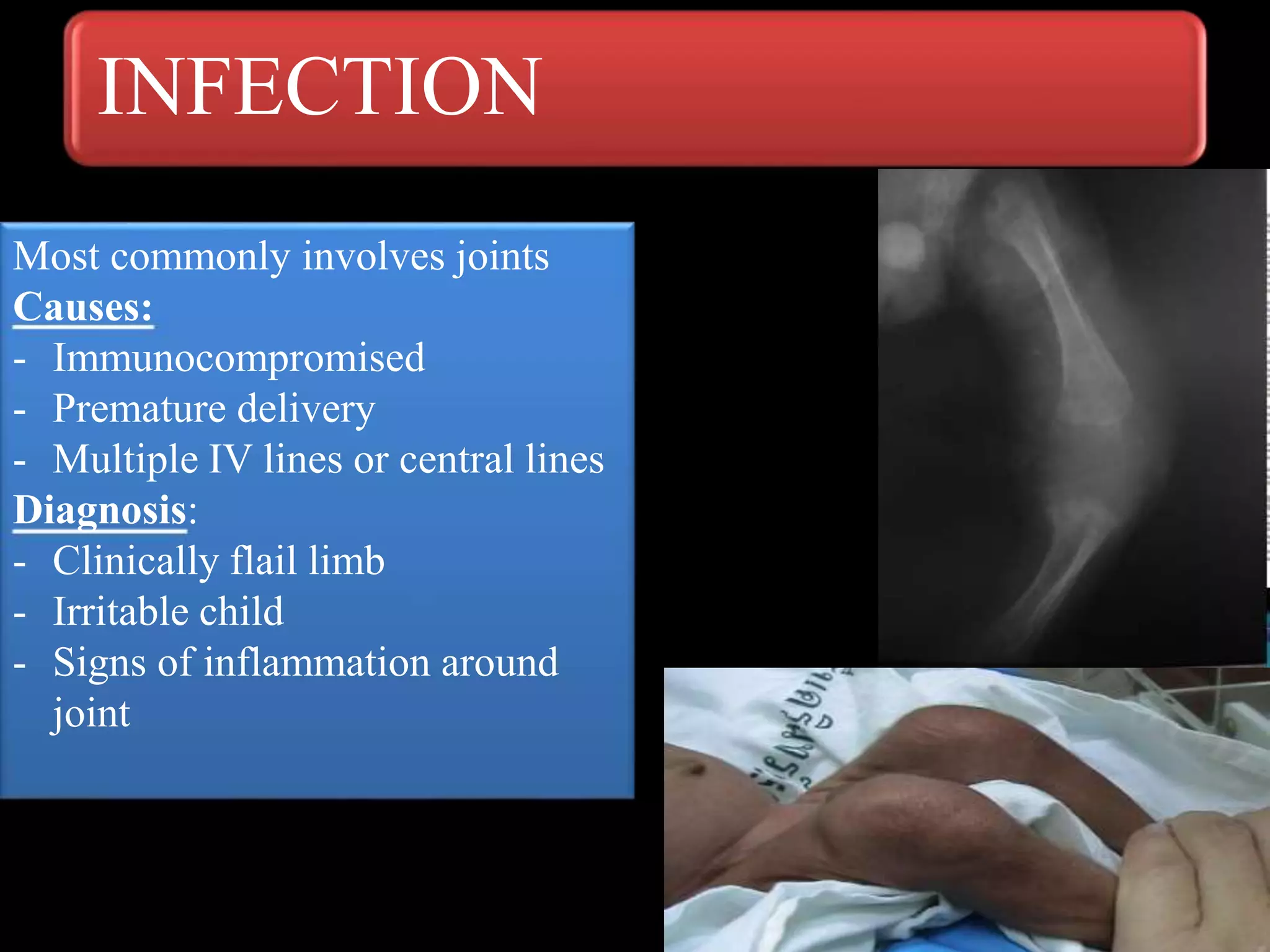
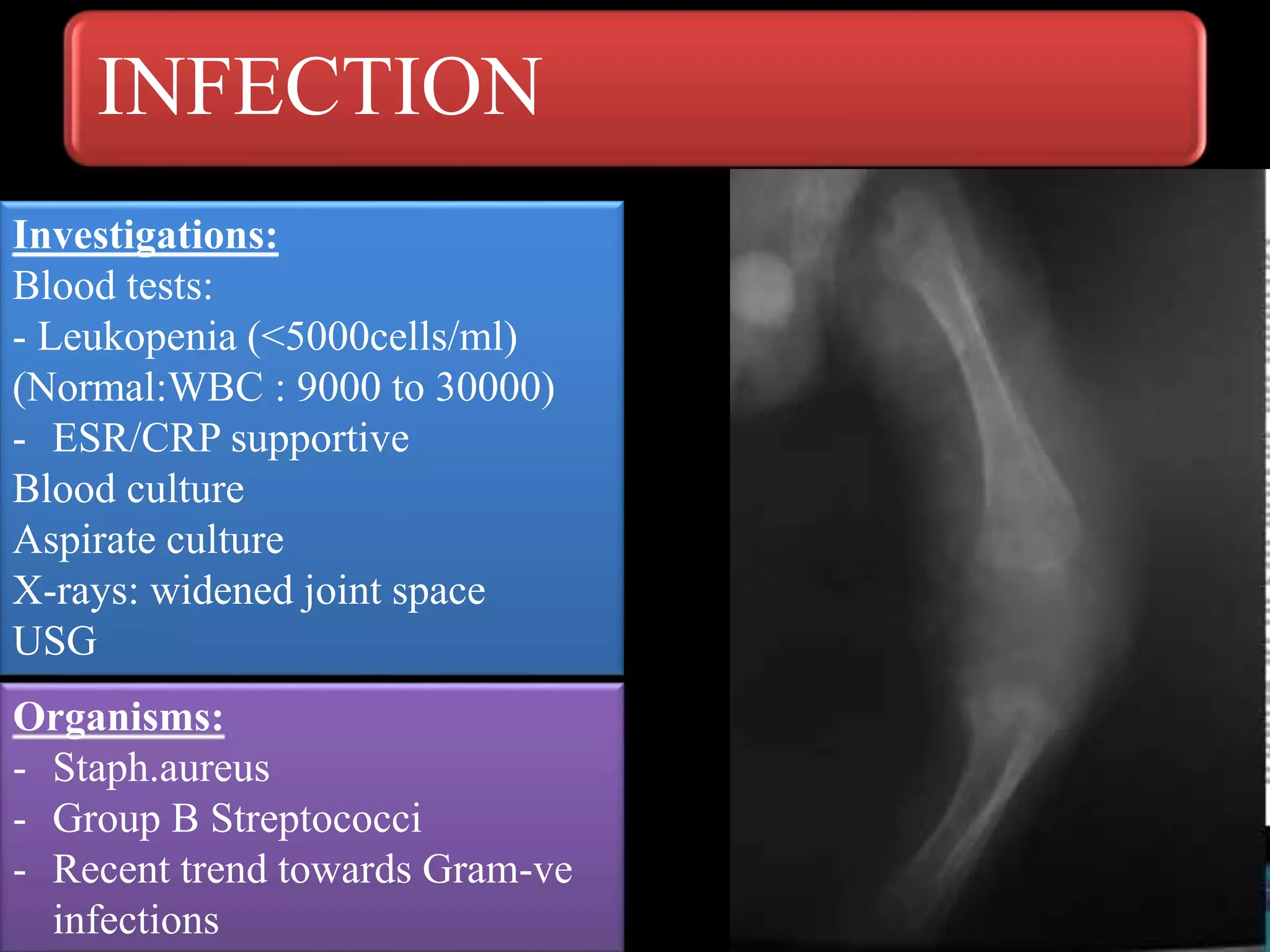
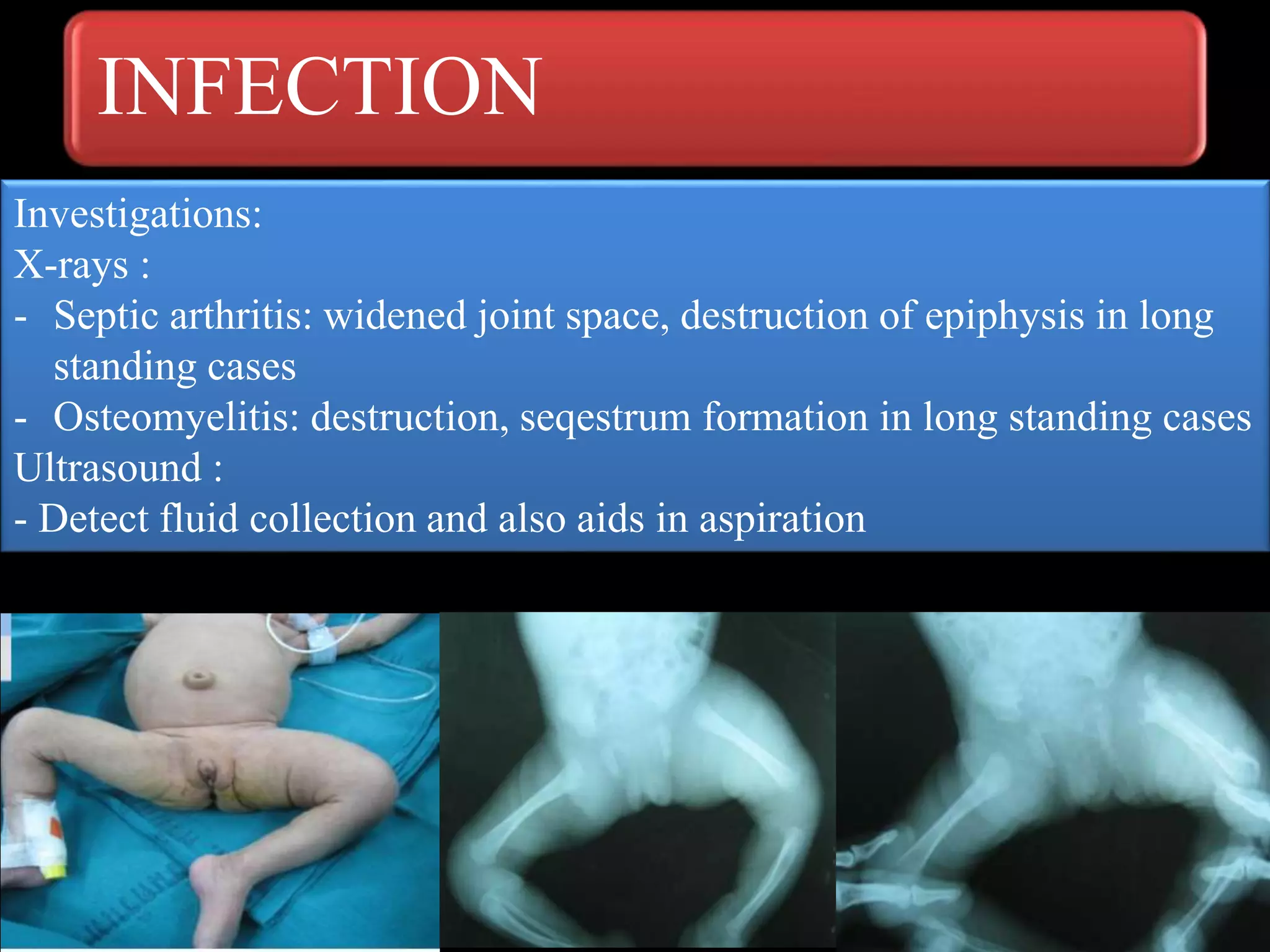


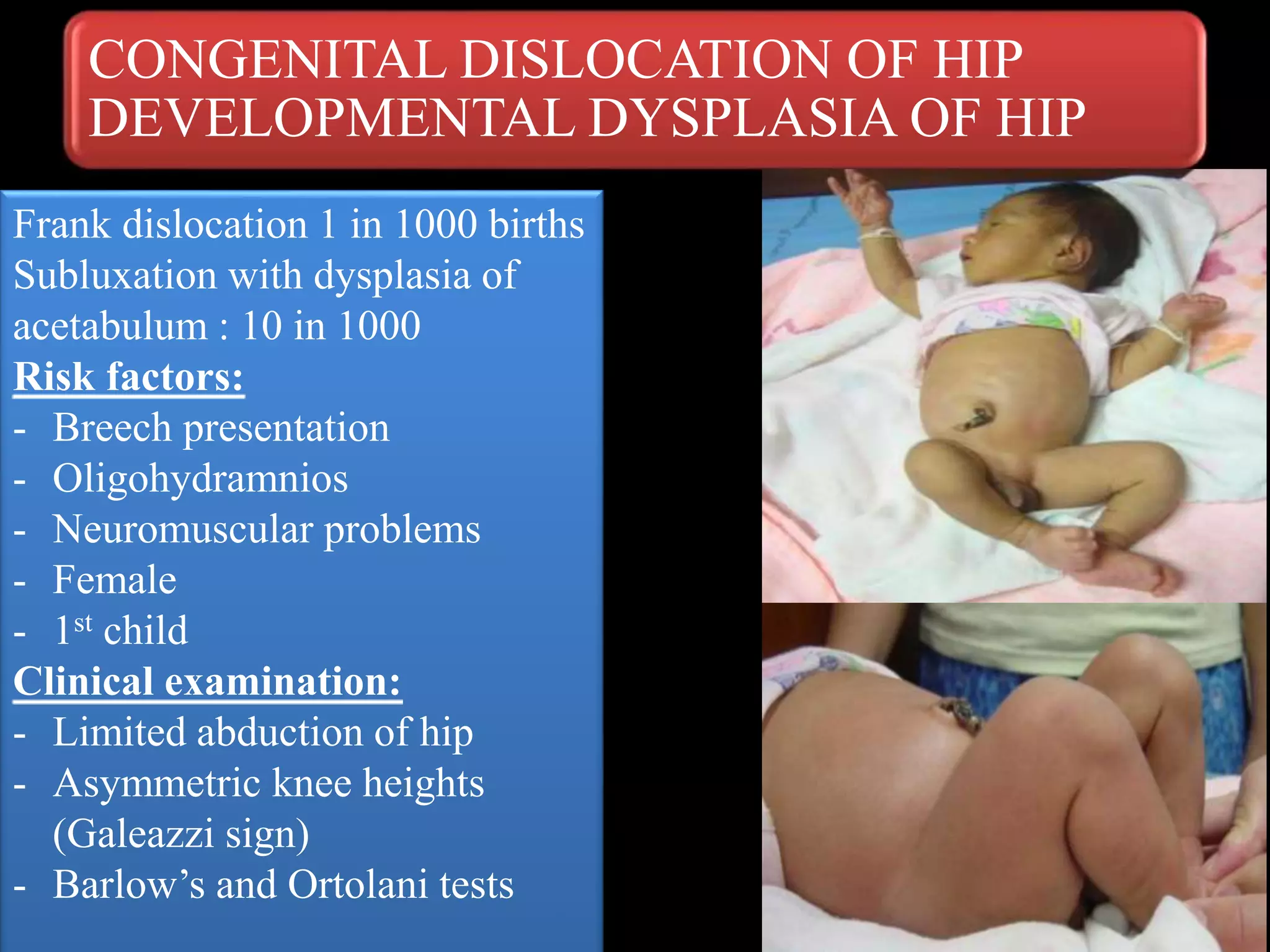

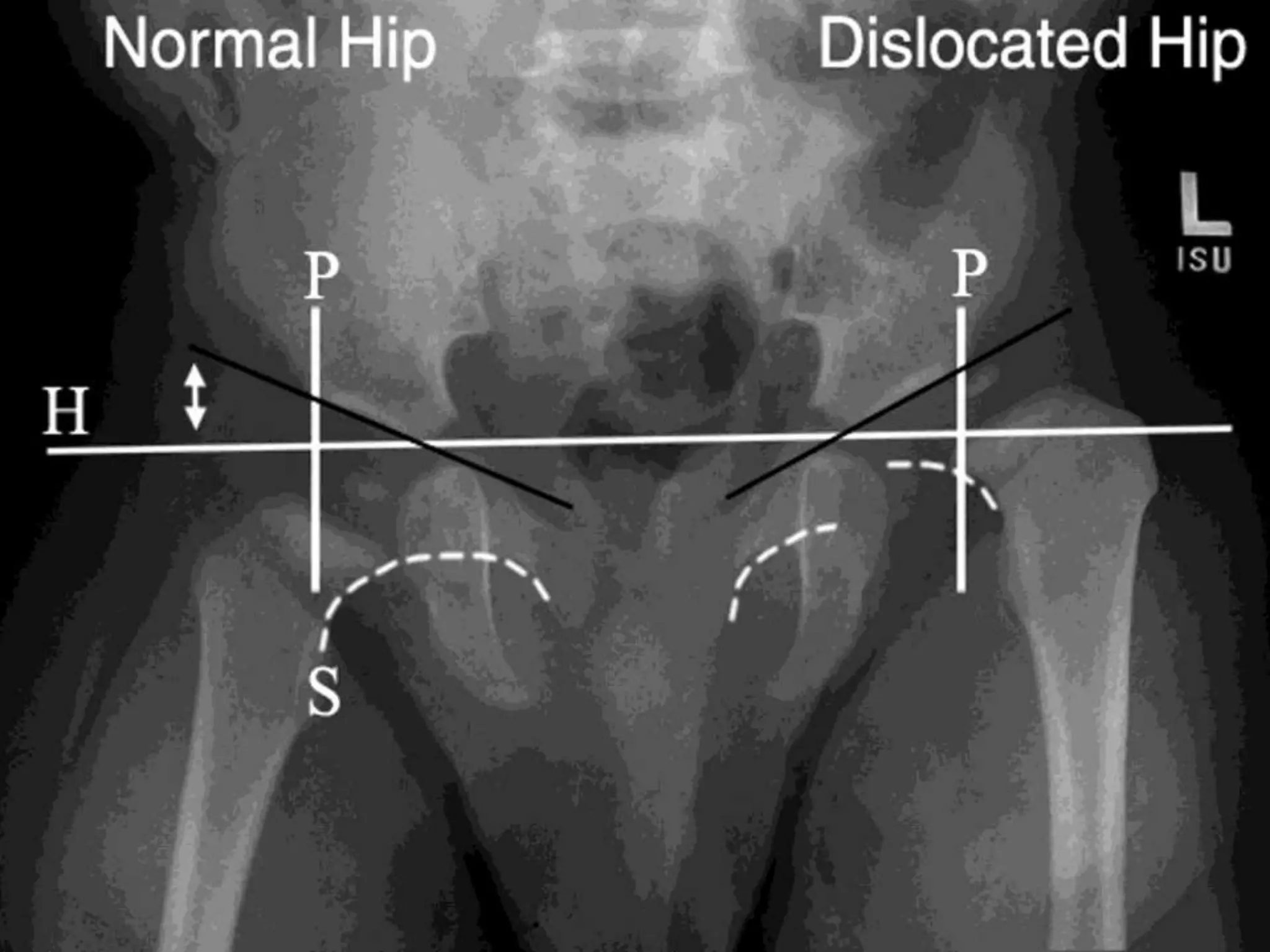







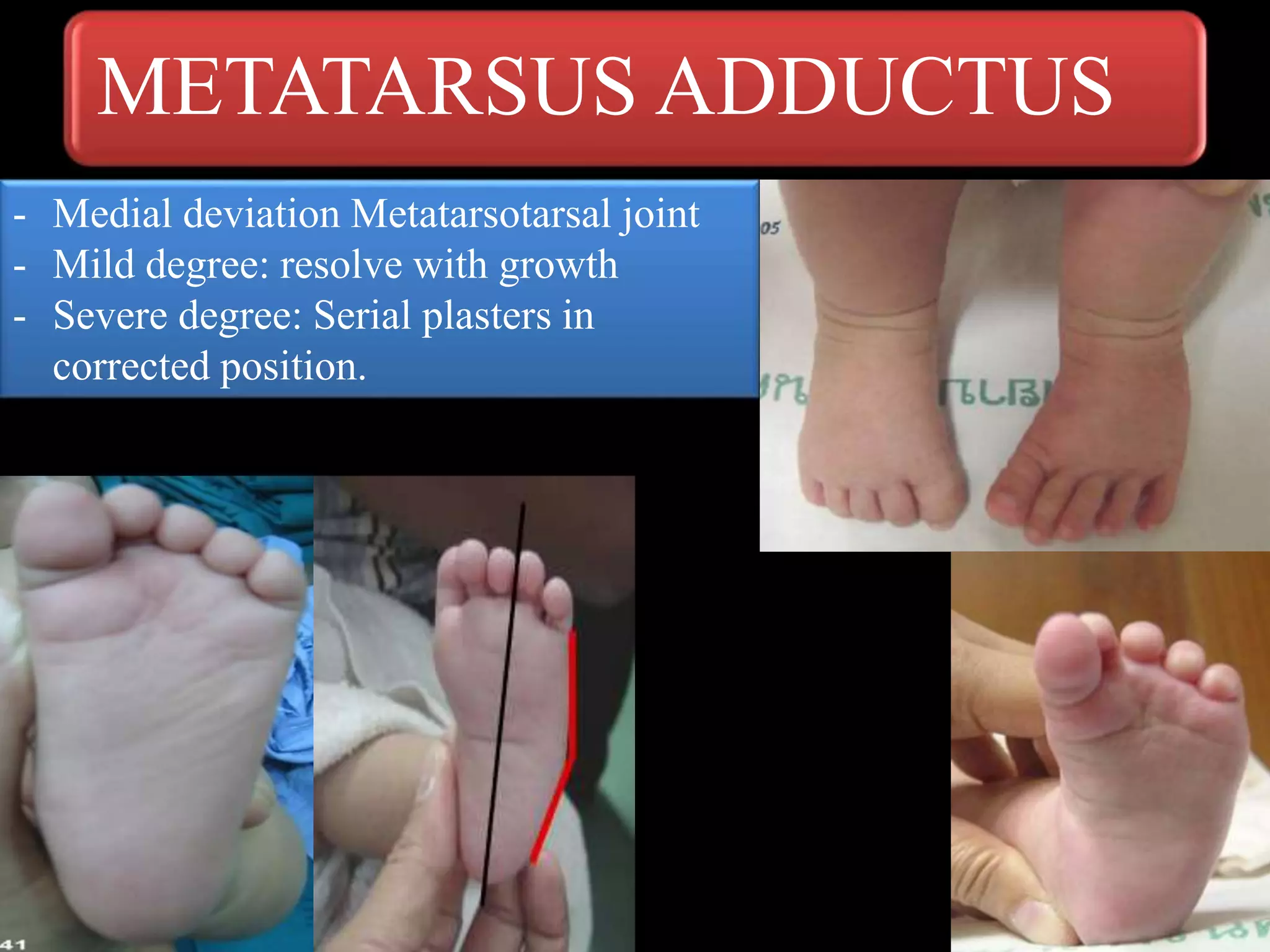
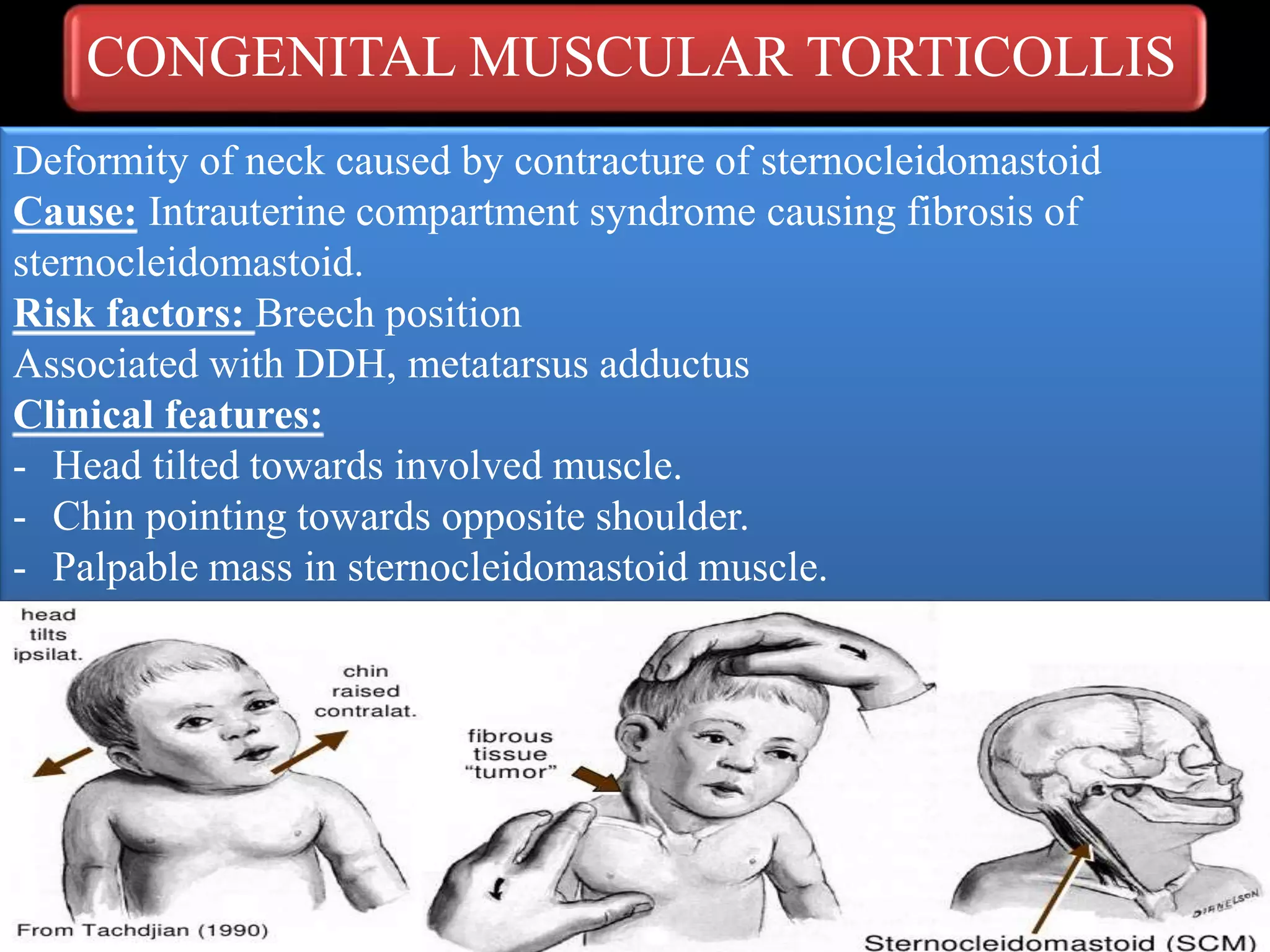

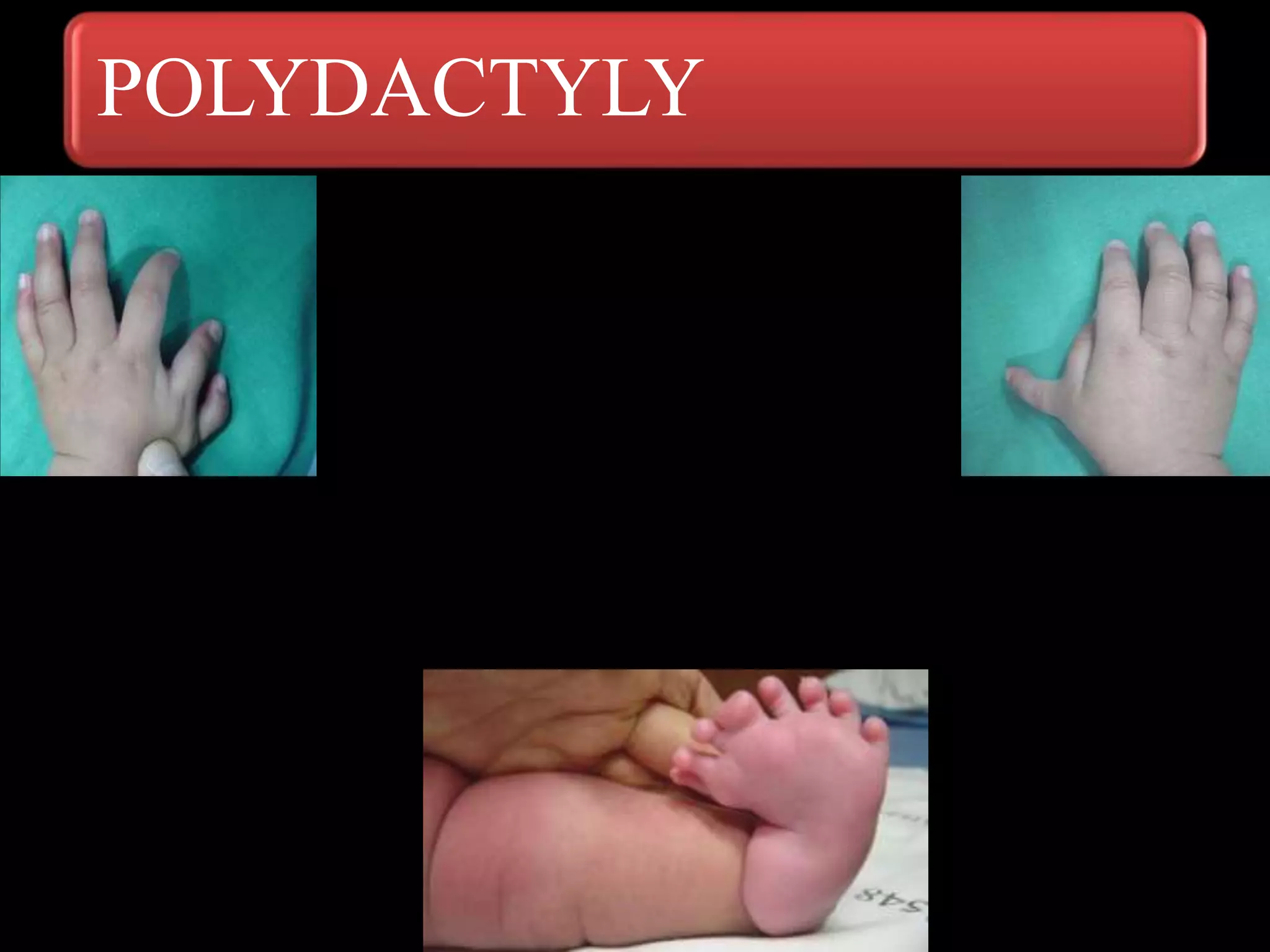



The document discusses various orthopedic problems in newborns, covering conditions such as birth-related fractures, infections, brachial plexus palsy, congenital dislocation of the hip, and clubfoot. It outlines risk factors, clinical features, diagnosis methods, and management strategies for each condition. Emphasis is placed on early detection and appropriate treatment to ensure favorable outcomes for affected infants.























































































