

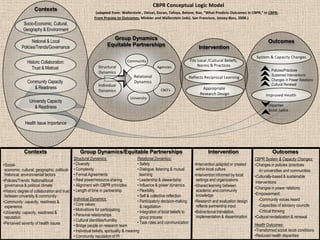
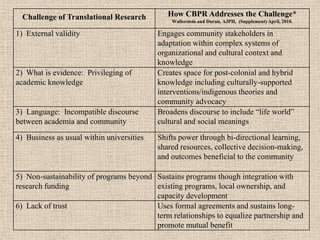
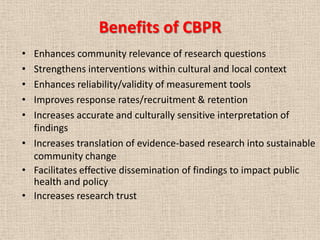
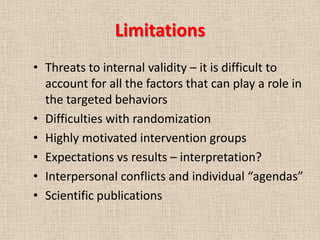


This document provides an overview of Community-Based Participatory Research (CBPR) including its history, principles, challenges, and benefits. Some key points: 1) CBPR aims to equitably involve community partners in all stages of research to address issues important to the community and promote social change. 2) Its roots trace back to action research and empowerment models that recognize communities as partners rather than subjects. 3) Challenges include balancing academic and community priorities, building trust over time, and ensuring research is culturally appropriate and sustainable. 4) Benefits include enhancing relevance, validity, translation and sustainability of research findings to improve community health.










































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











