Downloaded 365 times






![THEORETICAL MODELS
FOR RESOURCE
ALLOCATION
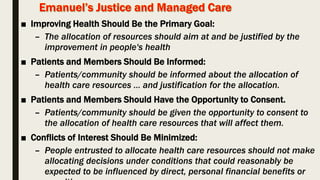
Ezekiel J. Emanuel" Justice and Managed Care: Four Principles for the Just Allocation of Health Care
Resources,” Hastings Center Report 30, no. 3 (2000): 8-16.
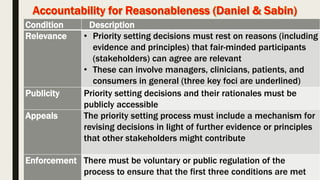
Daniels N, Sabin JE. The ethics of accountability in managed care reform. Health Aff (Millwood) 17[5],
50-64. 1998](https://image.slidesharecdn.com/publichealthethicskfmc-11-160514082441/85/Public-health-ethics-KFMC-11-05-2016-32-320.jpg)

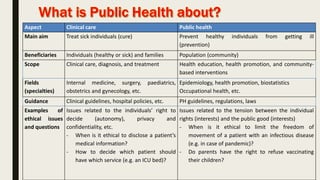
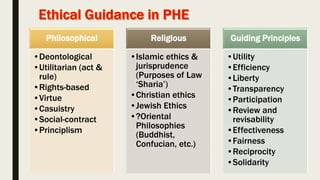
The document discusses the ethics of public health and health promotion, highlighting the differences between clinical care and public health practice, ethical issues in resource allocation, and dilemmas faced in public health interventions. It provides examples of ethical questions related to individual rights versus public good, privacy concerns, and resource allocation fairness, particularly during health crises. The content is informed by various ethical philosophies and frameworks, addressing the complexities of making ethical decisions in public health contexts.





















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















