Downloaded 693 times





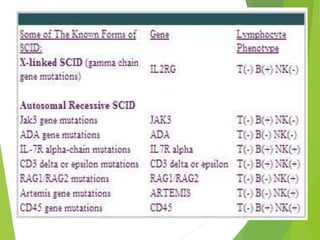





























Combined immunodeficiencies are disorders affecting multiple components of the immune system, leading to severe immune deficiencies. Severe combined immunodeficiency (SCID) is characterized by mutations that impede the functionality of T and B lymphocytes, resulting in increased vulnerability to infections, particularly in infants. Various types of SCID exist, including X-linked and autosomal recessive forms, and while genetic factors play a significant role in inheritance, treatments such as bone marrow transplants and gene therapy are under investigation.



















































































