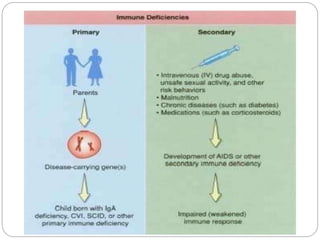
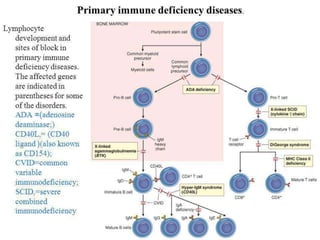
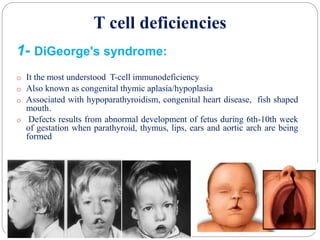
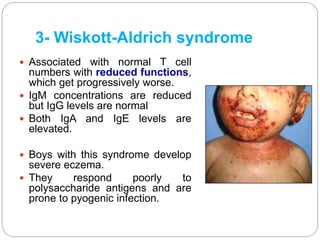
This document provides an overview of immunodeficiency. It begins by defining immunodeficiency and classifying it into primary and secondary types. Primary immunodeficiency is due to genetic defects present at birth, while secondary immunodeficiency is acquired from other diseases, infections, or medications. The document further discusses specific deficiencies in B cells, T cells, complement systems, and phagocytes. It also covers severe combined immunodeficiency and common secondary causes like infections, malnutrition, and immunosuppressive drugs or therapies. Treatment options include supportive therapies with antibiotics or immunoglobulin replacement as well as definitive therapies like bone marrow transplantation or gene therapy.