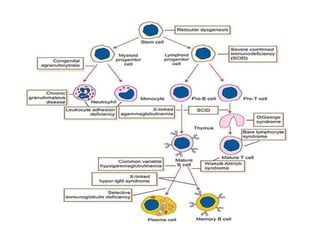
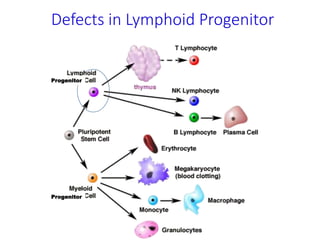
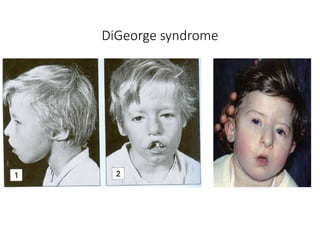
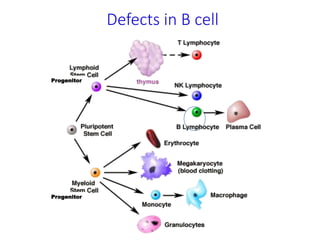
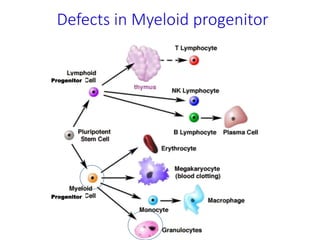
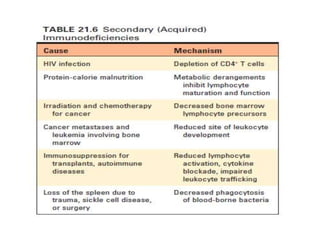
The document discusses immunodeficiency, which is a defect in the immune system that leads to failure to protect against disease. It describes primary/congenital immunodeficiency caused by genetic defects impairing immune system development or function. Secondary/acquired immunodeficiency is caused by factors like cancer treatment, burns, aging or HIV infection damaging immune cells. Specific primary immunodeficiencies discussed include combined antibody and T-cell deficiencies, T-cell deficiencies like DiGeorge Syndrome, and B-cell deficiencies like X-linked agammaglobulinemia. Defects can occur in hematopoietic stem cells, lymphoid progenitors or individual immune cell types.




















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















