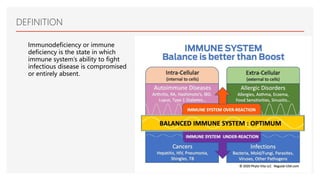
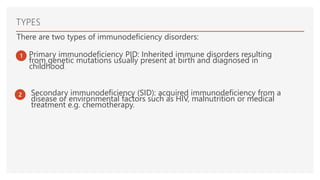
This document discusses immunodeficiency diseases. It defines immunodeficiency as a state where the immune system's ability to fight infections is compromised or absent. There are two types: primary immunodeficiency which is inherited and diagnosed in childhood, and secondary immunodeficiency which is acquired from diseases or environmental factors like HIV. Primary immunodeficiencies are classified into humoral deficiencies, cellular deficiencies, combined deficiencies, complement disorders, and phagocytosis disorders. Examples like X-linked agammaglobulinemia and common variable immunodeficiency are described. Nursing management focuses on infection assessment, patient teaching, and supportive care.