1) Tuberculosis of the spine, also known as Pott's disease, most commonly affects the thoracolumbar region of the spine in children and young adults.
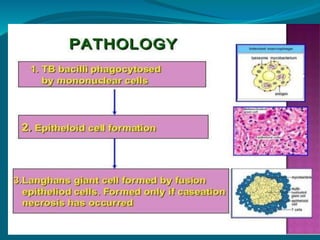
2) It spreads via hematogenous route from other sites like the lungs or intestines. The bacteria spreads through the venous plexus around the spine, causing granulomatous inflammation that can destroy vertebral bodies.
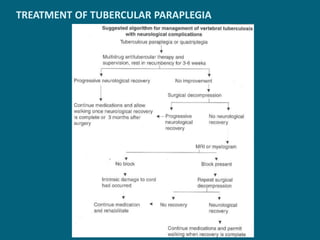
3) Clinical features include back pain, stiffness, deformities like gibbus or kyphosis, and cold abscesses that can track along tissues planes. Diagnosis involves imaging tests like x-rays, CT scans and MRI, while treatment consists of anti-tubercular drugs along with surgery in cases of parap