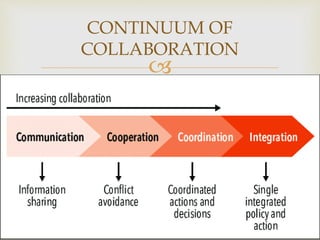
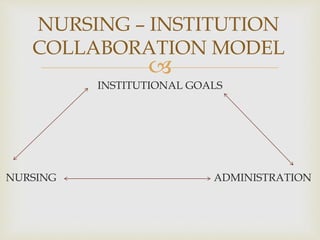
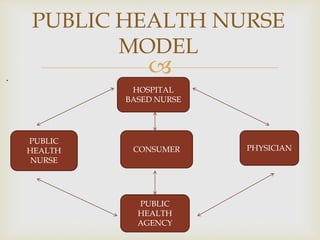
This document defines collaboration and discusses its importance in nursing. It provides definitions of collaboration from nursing theorists Virginia Henderson and Baggs and Schmitt. The document outlines the need for collaboration between nursing education and hospital nursing due to gaps in practical skills among new graduates. It discusses objectives, principles, characteristics, phases and types of collaboration, as well as issues that can impact collaboration within and outside of nursing. The document also summarizes several models of clinical education that aim to strengthen collaboration between academia and clinical practice settings.
















































![7936 different models of collaboration between nursign education and service [1]](https://cdn.slidesharecdn.com/ss_thumbnails/7936differentmodelsofcollaborationbetweennursigneducationandservice1-110627040119-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)











































