Downloaded 731 times






This document discusses various models of collaboration within nursing and between nursing and other professions. It begins by defining collaboration and exploring the historical relationship between nurses and physicians. Several models of collaboration are presented, including the traditional practice model, nursing-institution collaboration model, public health nurse model, nurse-community collaboration, and nurse-physician collaborative practice model. The document also discusses collaboration with assistive personnel, interdisciplinary collaboration, and collaboration in advanced nursing practice. It explores various skills needed for effective collaboration and ways nurses can act as collaborators. Overall, the document provides an overview of the concepts of collaboration within the nursing profession and with other health professionals from both a theoretical and historical perspective.
An introduction to collaboration issues within and outside nursing, focusing on the significance of working together in healthcare.
Defines collaboration, highlighting a partnership among healthcare providers and objectives like client-centered care and improved satisfaction.
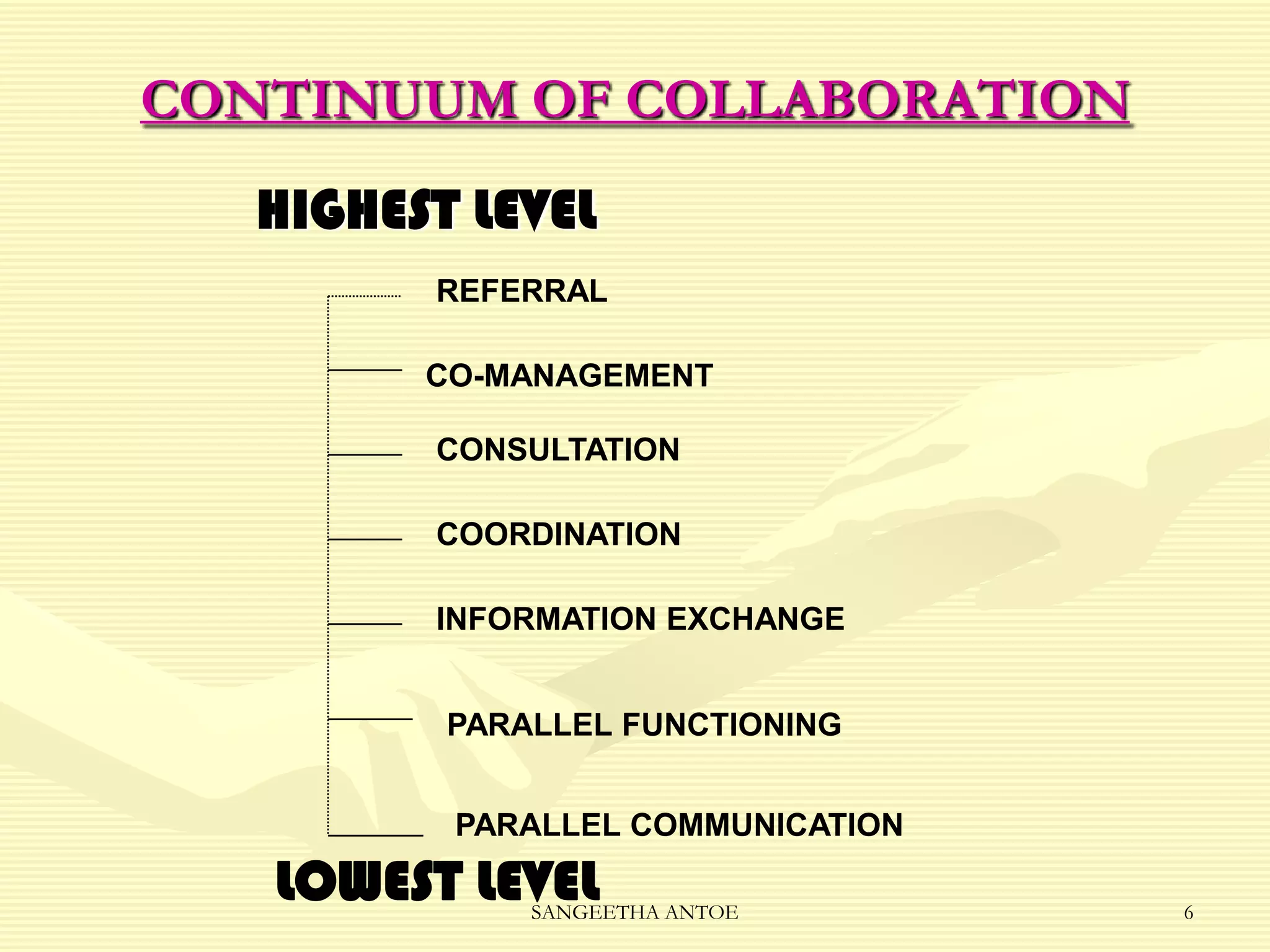
Illustrates the continuum of collaboration from highest to lowest levels, including referral, co-management, and information exchange.
Outlines key principles of collaboration: accountability, mutual agreements, and reciprocal respect among partners.
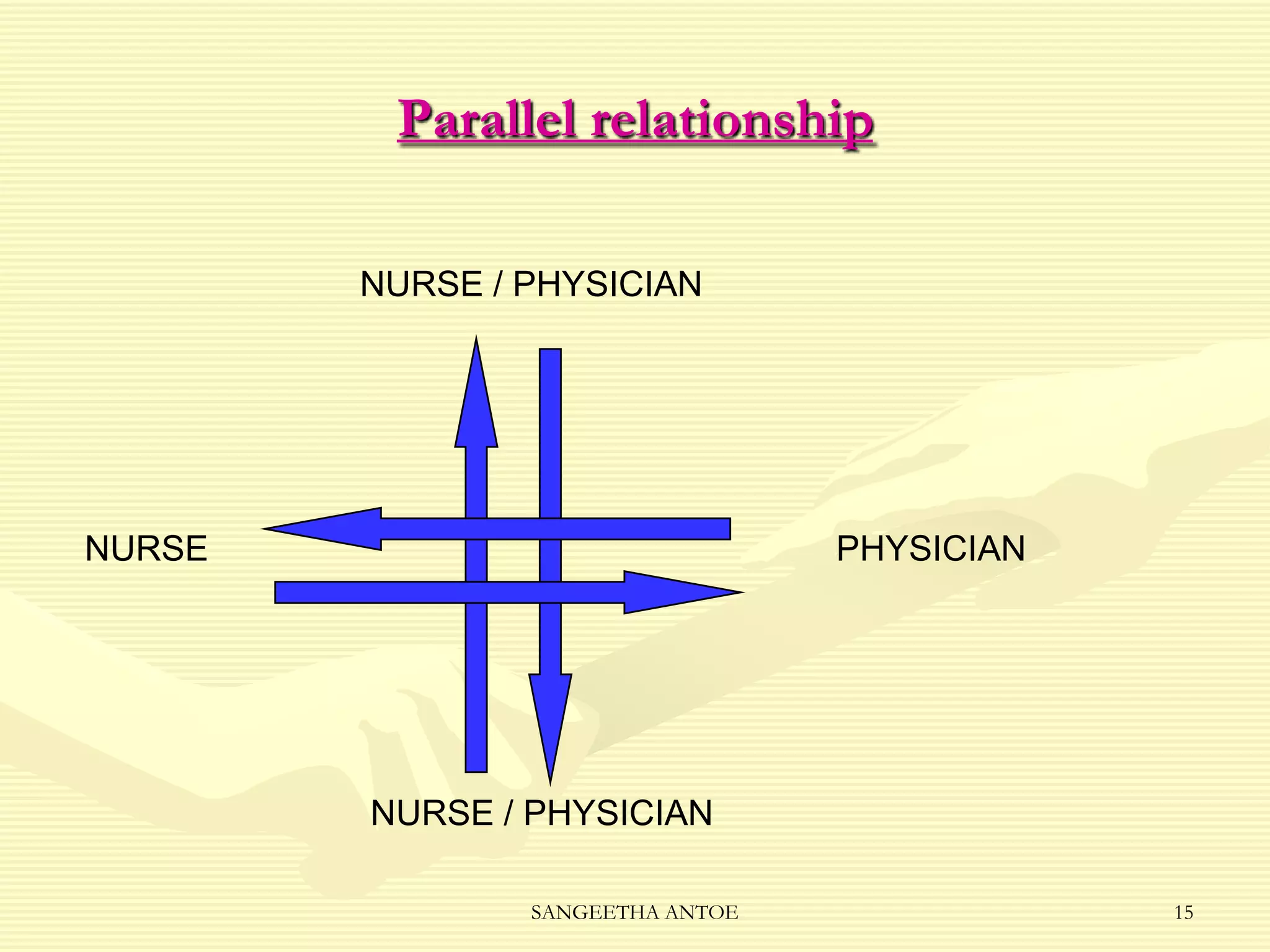
Describes the three types of relationships in healthcare: complementary, symmetrical, and parallel relationships.
Explains the dynamics of a complementary relationship where one participant dominates, affecting creativity and independence.
Details the symmetrical relationship where control is balanced, sharing power enhances communication.
Outlines how control shifts between participants in a parallel relationship, ensuring effective and flexible communication.
Introduction to various collaborative models in nursing and healthcare.
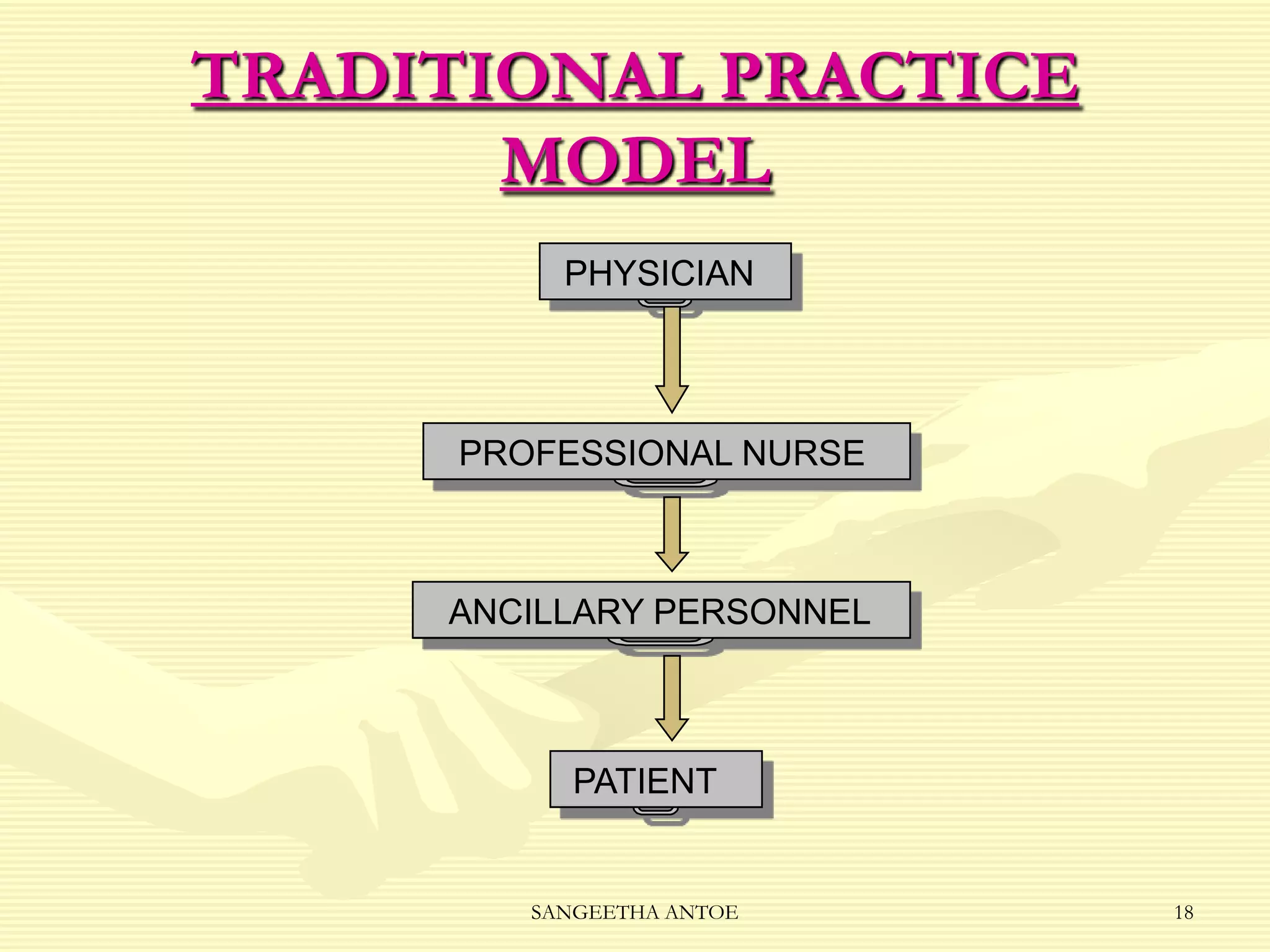
Details the traditional practice model where authority is hierarchical, and communication is fragmented.
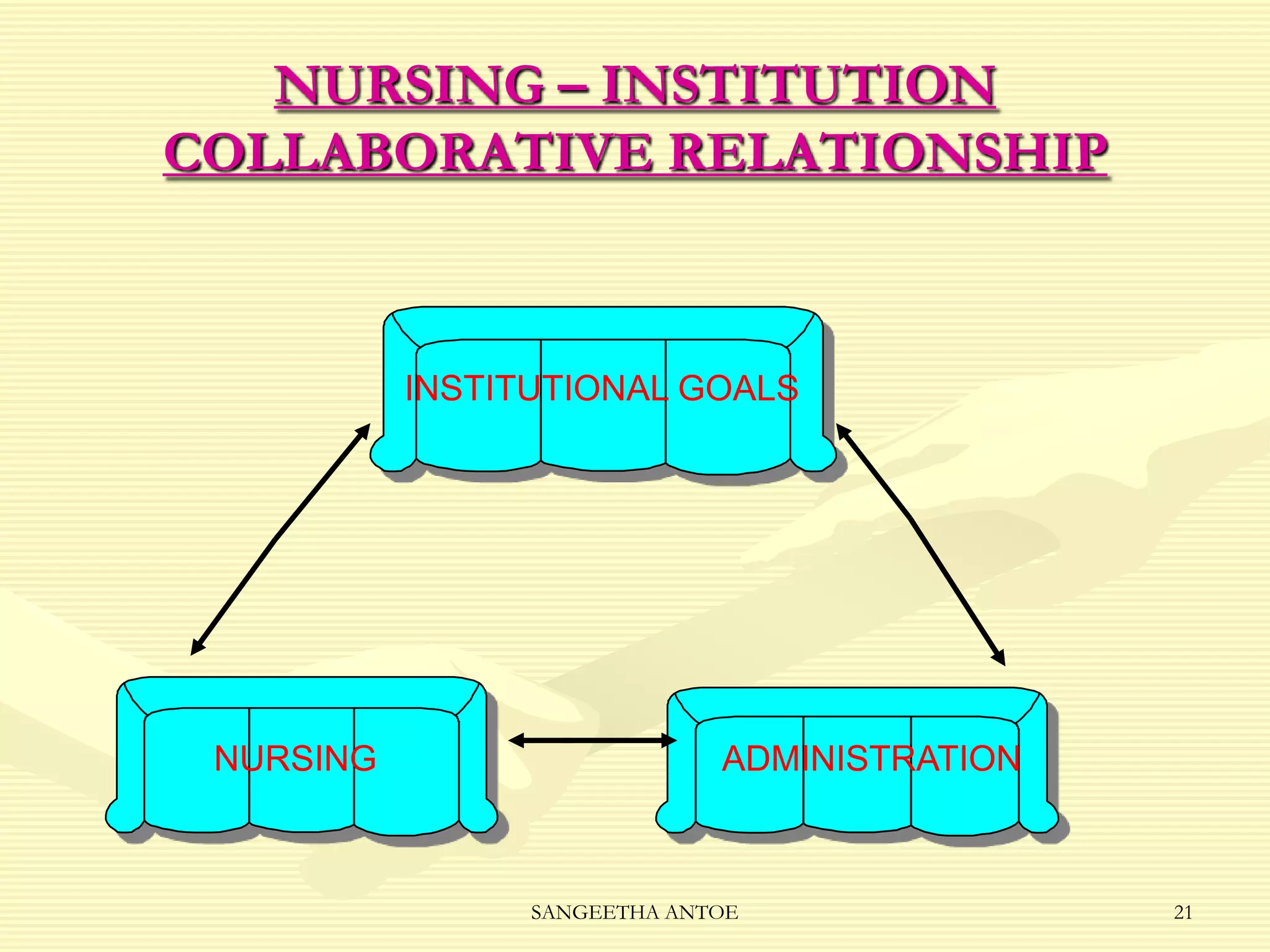
Focuses on collaboration between nursing and institution to enhance patient care through integrated plans.
Describes the collaboration between clinical nurse specialists and educators for curriculum development.
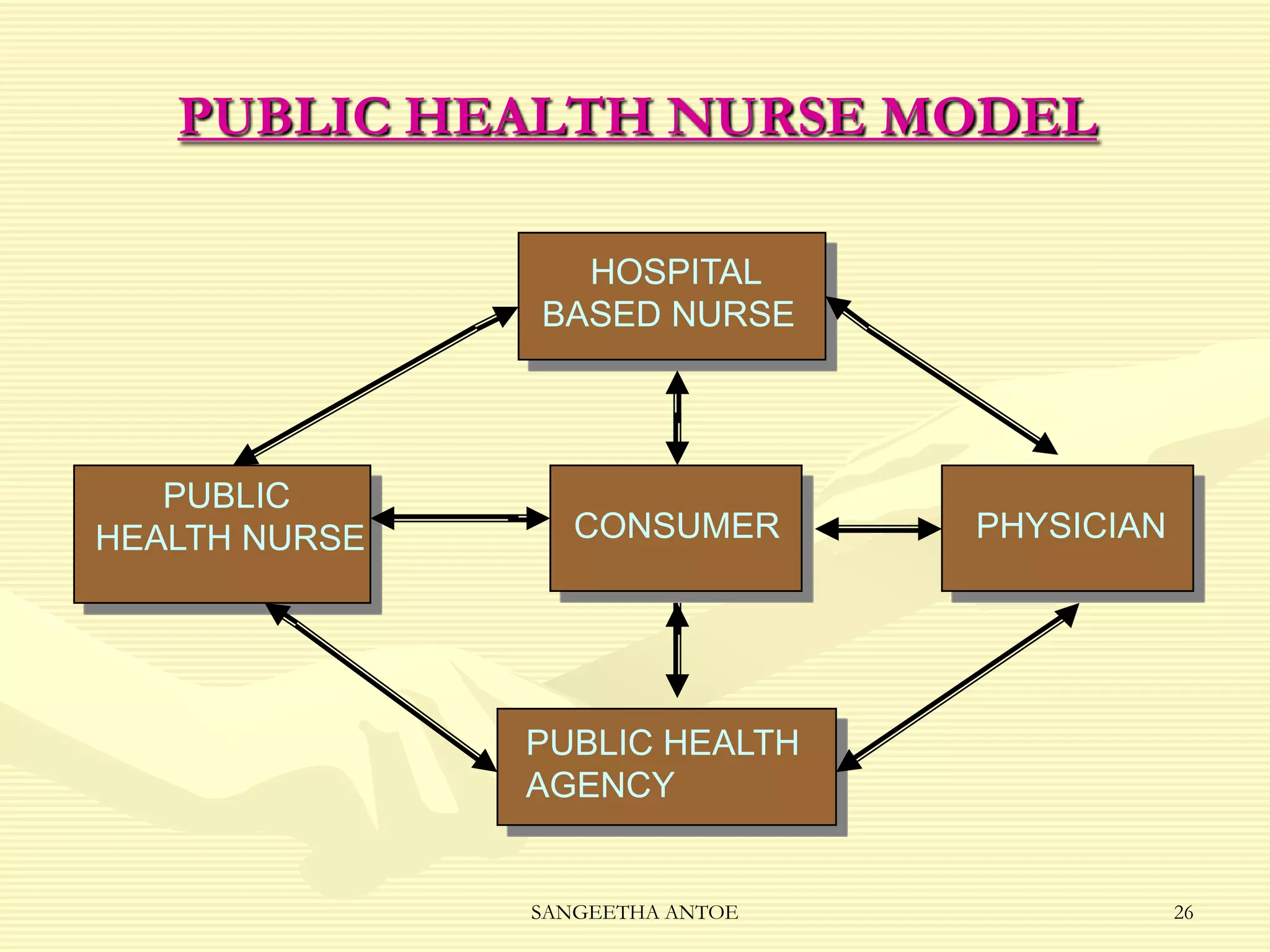
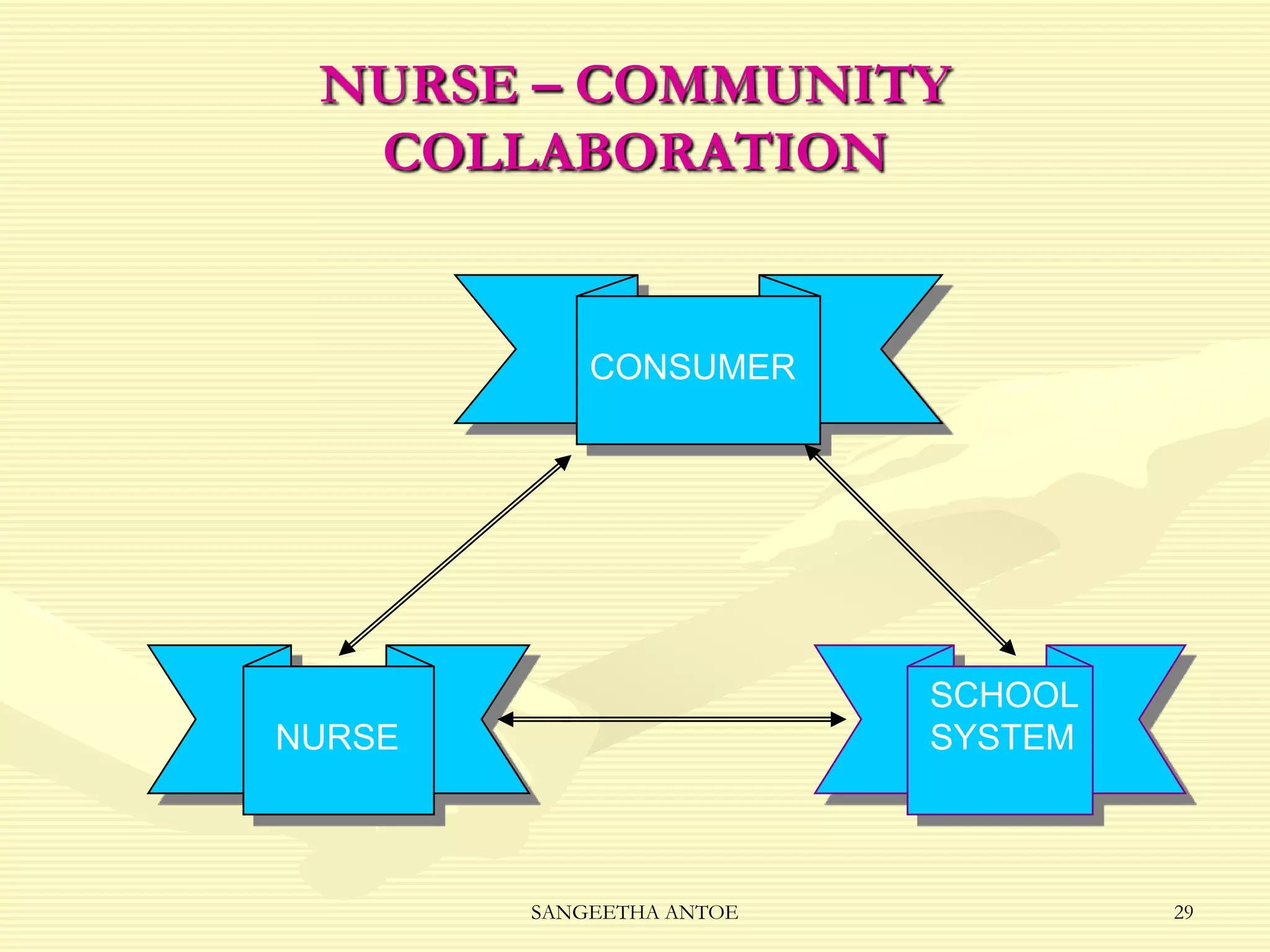
Illustrates the public health nursing model emphasizing communication between various stakeholders for effective care.
Highlights the nurse's role in community collaboration for comprehensive care and maintaining quality.
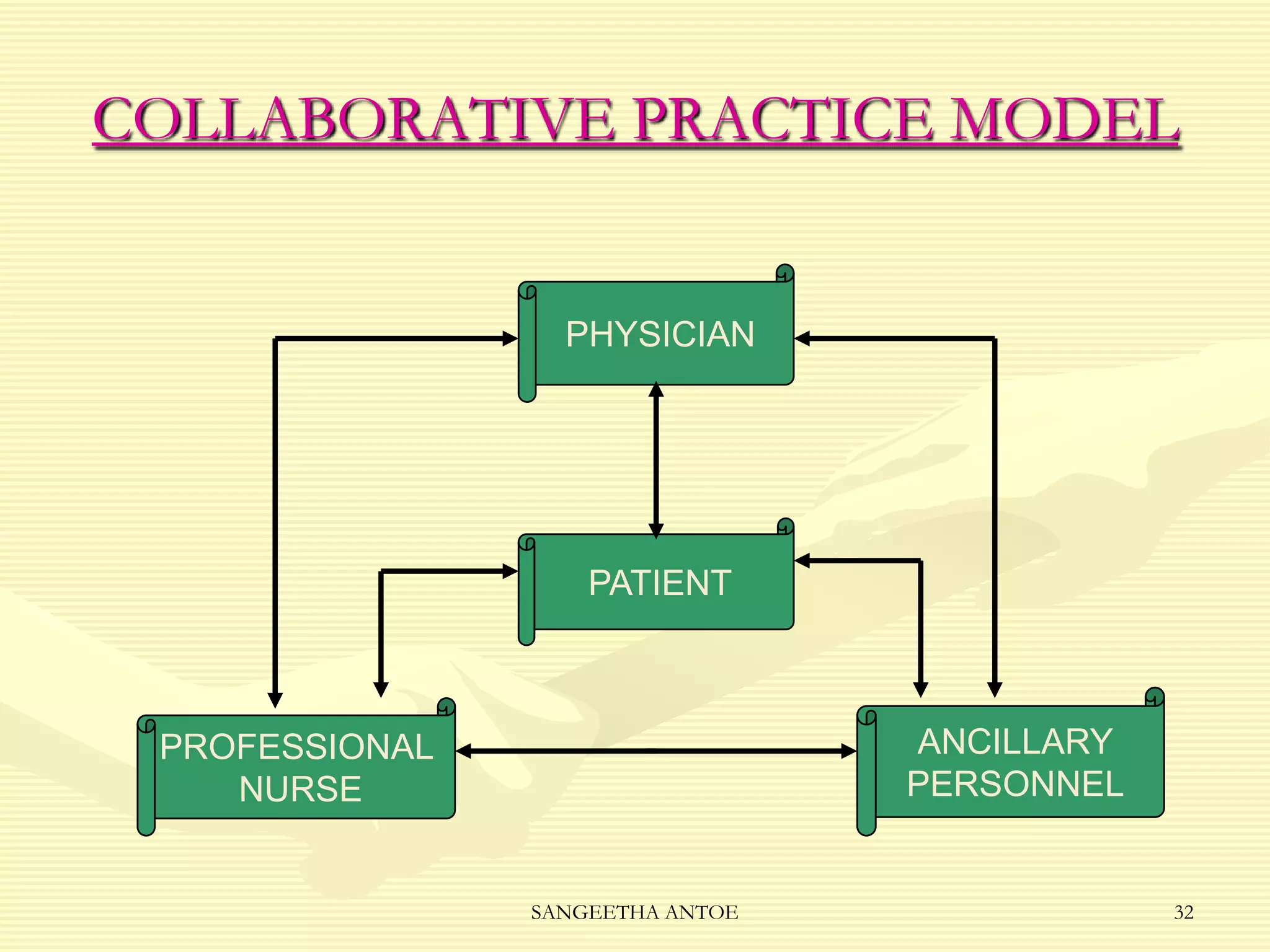
Discusses the historical context of nurse-physician collaboration in healthcare, leading to improved care quality.
Presents key research findings encouraging nurses' decision-making and recognizing the importance of teamwork.
Emphasizes the significance of interdisciplinary collaboration to enhance healthcare effectiveness.
Presents research findings on the impacts of interdisciplinary collaboration on patient readmission rates.
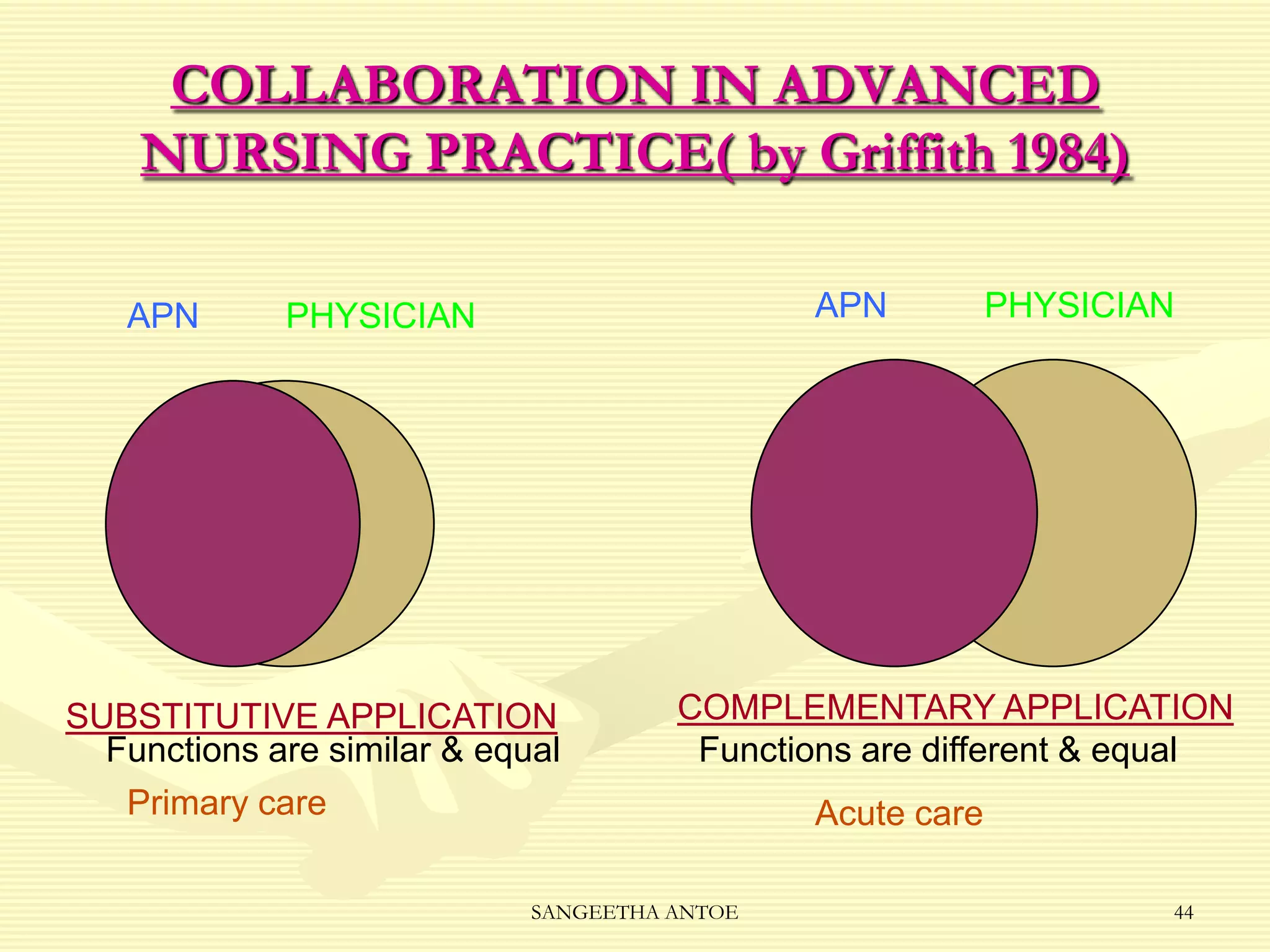
Describes the collaborative practice model in advanced nursing, focusing on roles beyond their standard scope.
Explains a model promoting teamwork between students, faculty, and staff to enhance learning and patient care.
Discusses how a collaborative team approach improves communication and productivity across disciplines.
Describes a pilot project aimed at improving patient care quality through academic leadership and collaboration.
Details the dual role of the head of nursing in providing leadership in both academic and practical settings.
Discussion on the Rush model where nursing leadership integrates care, education, and research efforts.
Highlights essential collaborative skills necessary for effective teamwork and enhancing healthcare delivery.
Details the collaborative role of nurses with clients and peers in healthcare decisions and quality care.
Discusses nurses’ collaborations with professional organizations and legislators to influence healthcare policy.
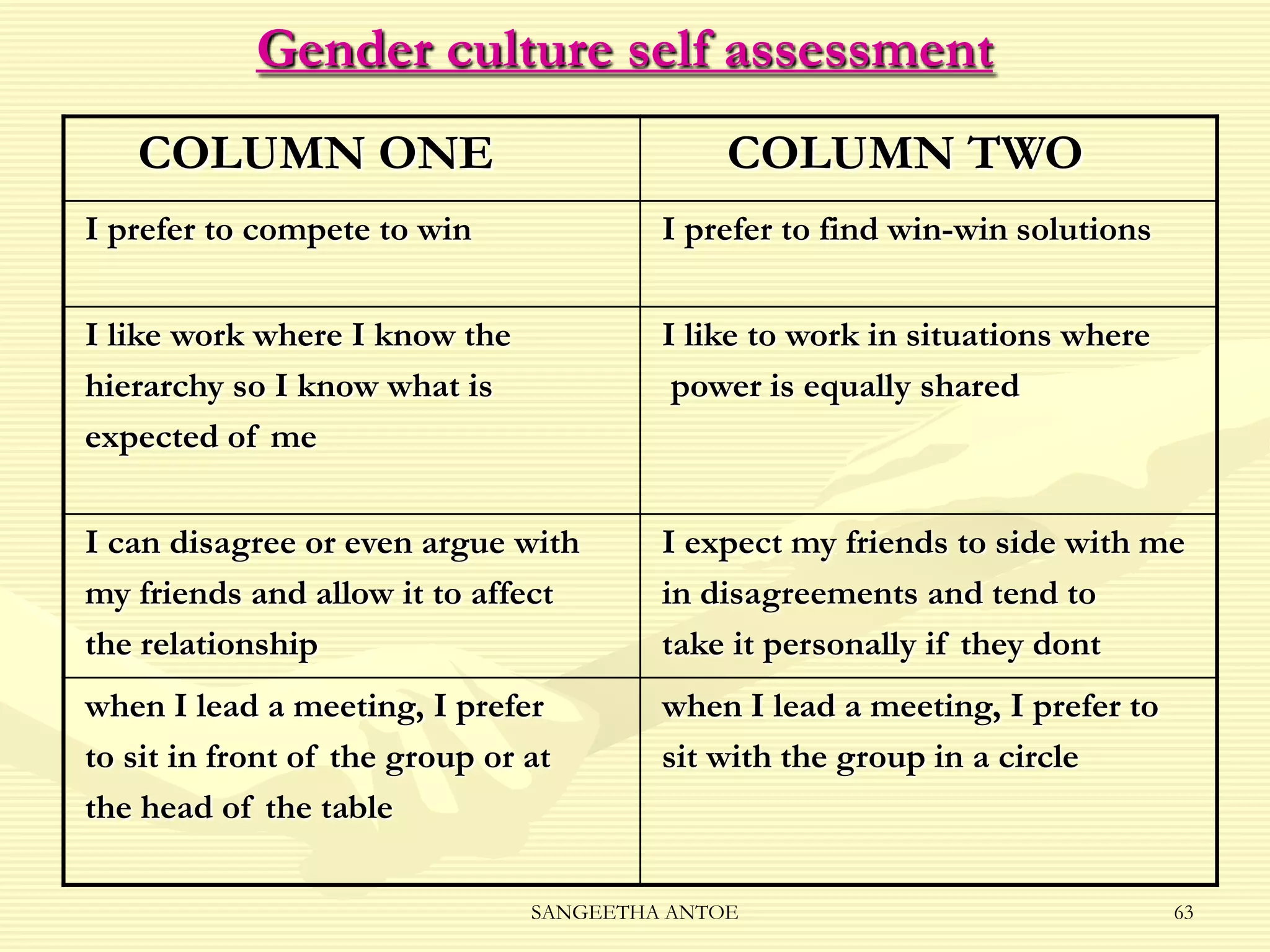
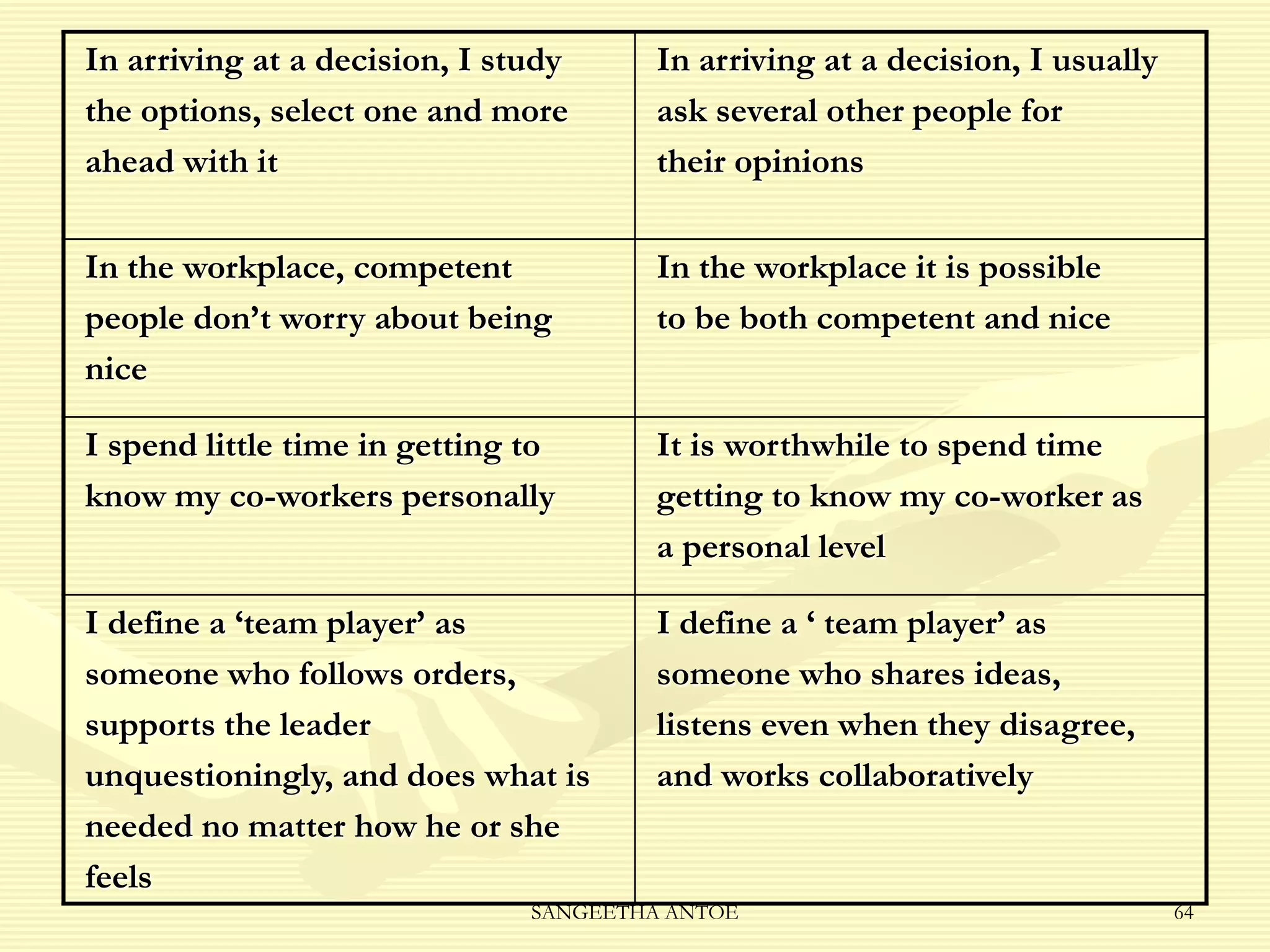
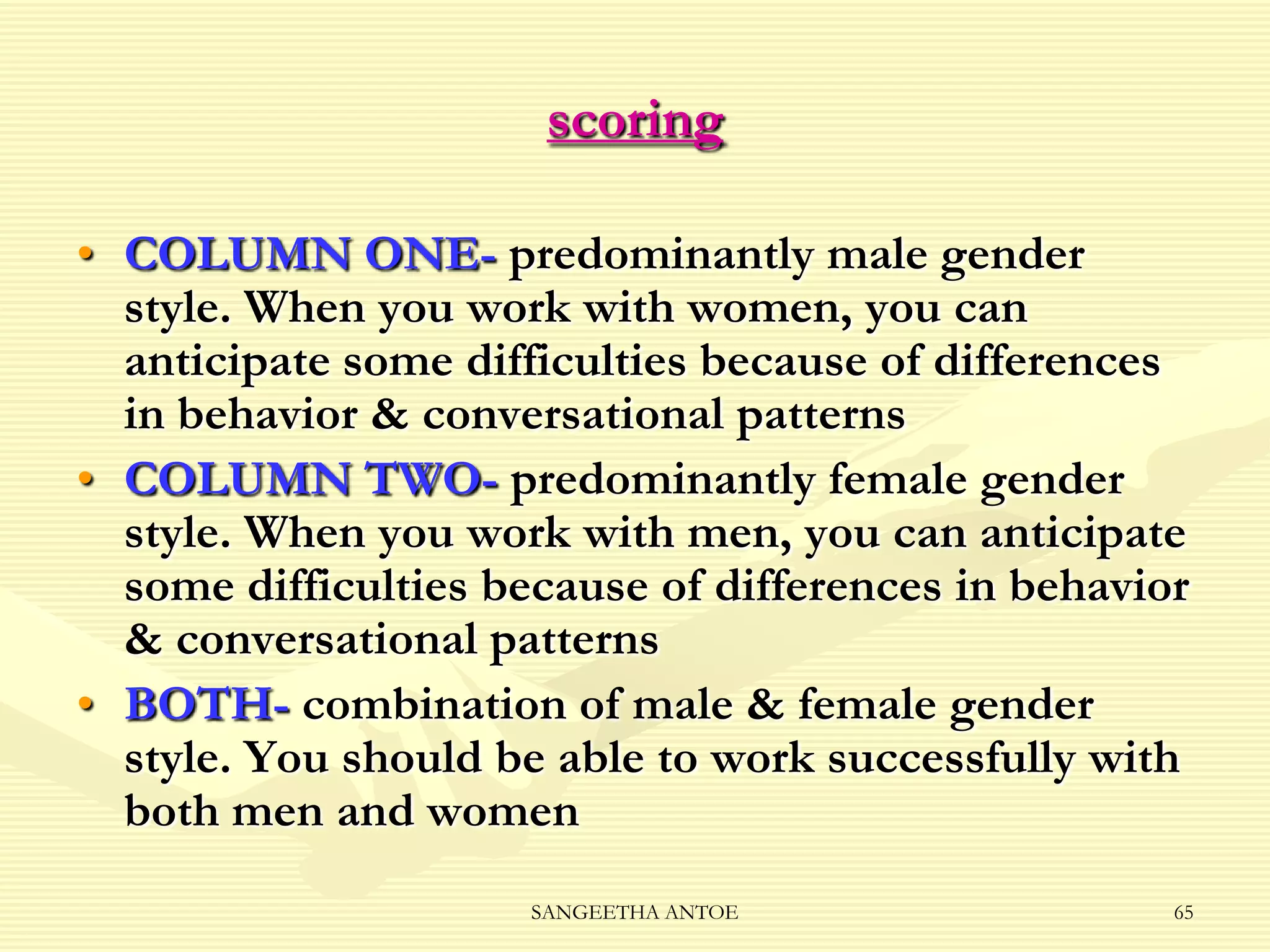
Introduces a self-assessment tool to aid understanding of gender-based communication styles in collaboration.
Wraps up the presentation, reiterating the theme of collaboration in nursing.


































![7936 different models of collaboration between nursign education and service [1]](https://cdn.slidesharecdn.com/ss_thumbnails/7936differentmodelsofcollaborationbetweennursigneducationandservice1-110627040119-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































