
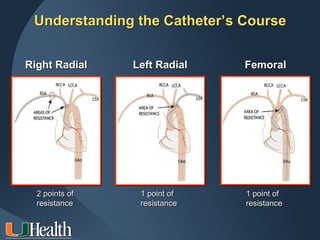
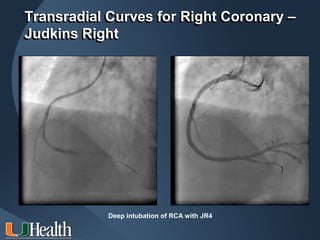
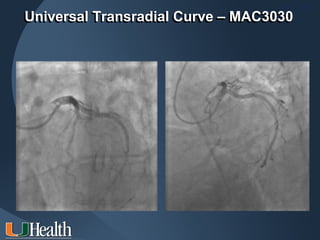
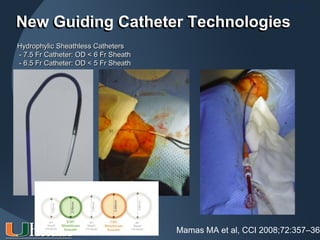
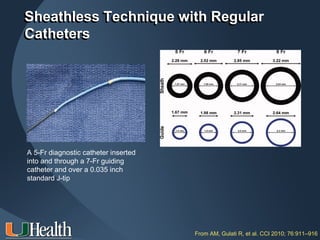


This document discusses catheter selection for transradial procedures, including right and left heart catheterization. It describes the different points of resistance encountered with right versus left radial access. Various catheter curves are presented for accessing the right coronary artery, left coronary artery, and performing complex PCI through radial access. New technologies like hydrophylic sheaths and sheathless guiding catheters are also summarized. Proper catheter selection and technique are emphasized for successful transradial procedures.

























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










