
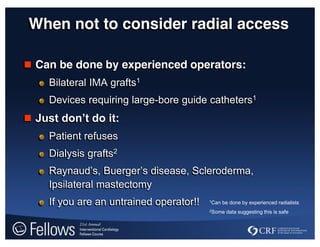




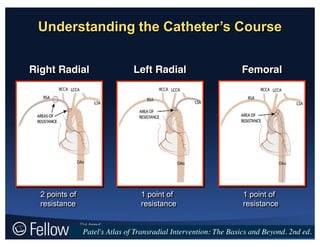















This document discusses techniques for transradial access and intervention. It begins by outlining three levels of competency for operators and discusses when radial access may not be appropriate. It then provides a step-by-step guide for radial access procedures, covering patient positioning, arterial puncture, navigating vascular anatomy, catheter selection, and hemostasis. Predictors of procedural failure are presented. The document concludes by providing tips for implementing a successful radial program.
























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















