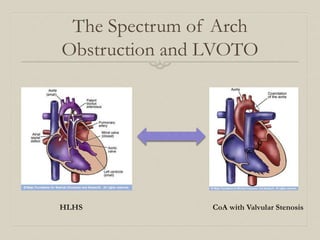
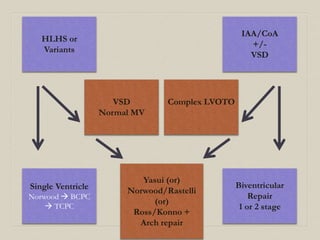
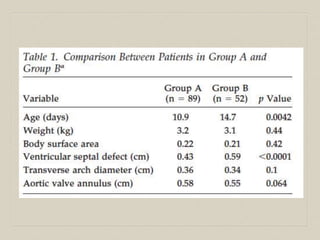
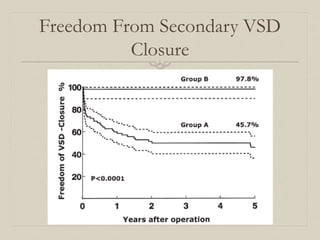
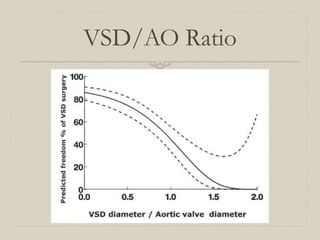
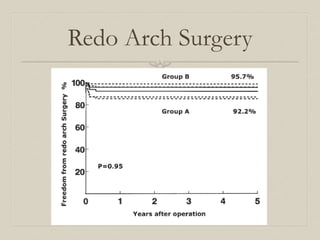
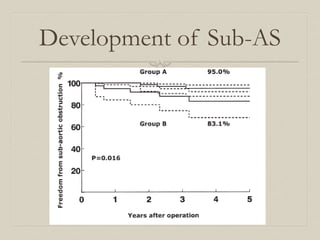
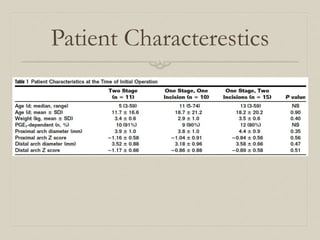
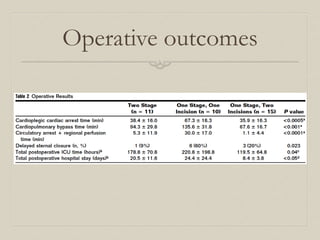
This document discusses the management options for coarctation of the aorta (CoA) accompanied by a ventricular septal defect (VSD). It outlines the associated lesions that can be present and the surgical repair approaches, which include single-stage full repair versus staged repair. A retrospective analysis of 141 neonates with CoA and VSD compared outcomes of staged repair versus full repair. The conclusion is that neonates with this condition need assessment for left ventricular outflow tract obstruction and that both primary and staged surgical approaches can have acceptable outcomes, with CoA repair alone preferred if the VSD may close spontaneously.

















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





