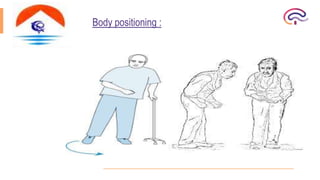






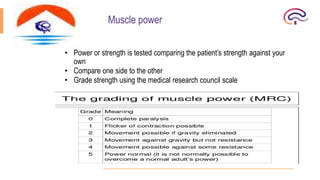



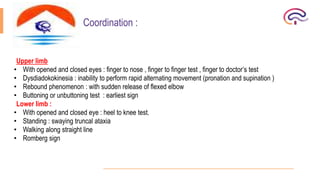


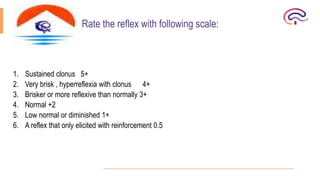





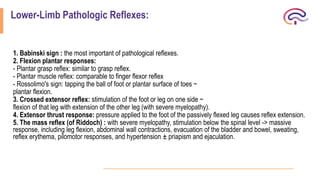




This document summarizes the steps for performing a thorough motor system examination. It outlines how to inspect muscles for wasting, deformities, involuntary movements, and trophic changes. It describes how to assess muscle tone, power, coordination, reflexes, and gait. Abnormal findings are defined, including pathological reflexes like Babinski's sign. The exam involves a full evaluation of muscle and nerve function in the upper and lower limbs as well as the trunk.























































































