
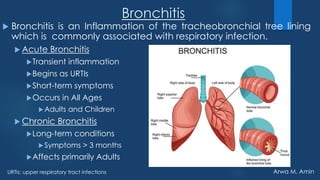
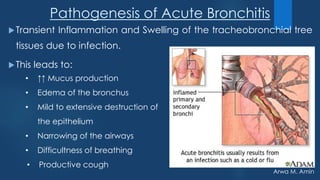
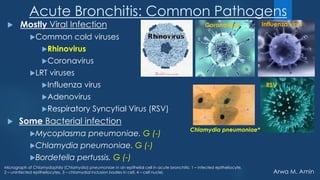


The document discusses lower respiratory tract infections (LRTIs) with a focus on bronchitis, its types (acute and chronic), and management strategies. It highlights the pathogenesis, common pathogens, risk factors, symptoms, and treatment options for both acute and chronic bronchitis, emphasizing the importance of symptomatic care and when antibiotics may be necessary. Additionally, it addresses the role of vaccinations in preventing complications related to these infections.




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








