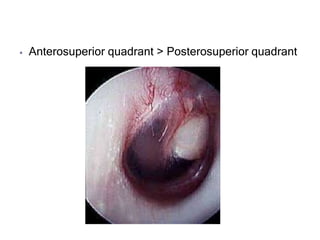
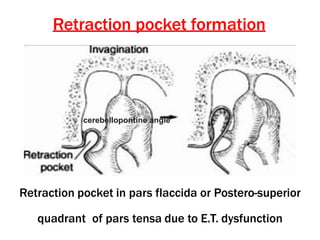
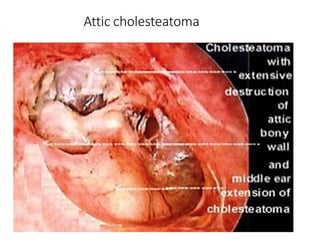
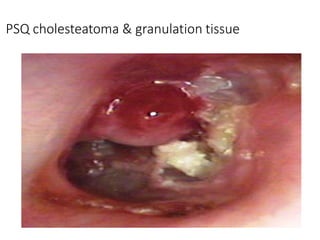
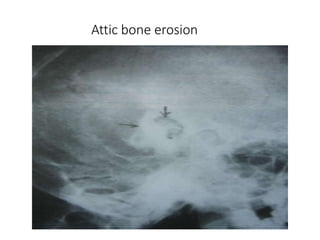
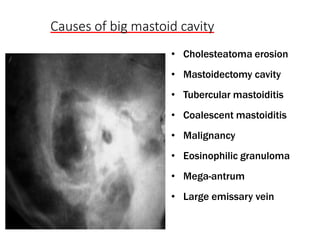
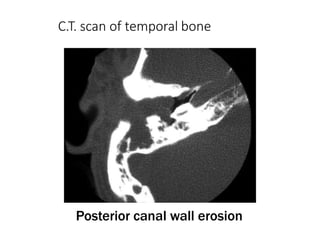
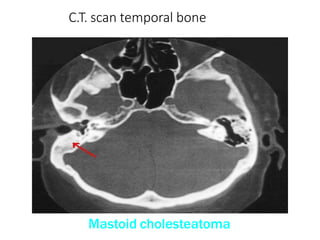
Chronic Suppurative Otitis Media with atticoantral disease, also known as COM-Squamous, is a chronic infection of the middle ear cleft lasting over 3 months with cholesteatoma and granulation tissue in the attic or posterosuperior quadrant of the eardrum. Key features include cholesteatoma, which is a sac of keratinizing squamous epithelium that grows at the expense of surrounding bone, potentially causing complications from bone erosion. Investigations include examination under the microscope, ear discharge culture and sensitivity, audiometry, CT scan and x-ray of the mastoid bone.