Download as PDF, PPTX
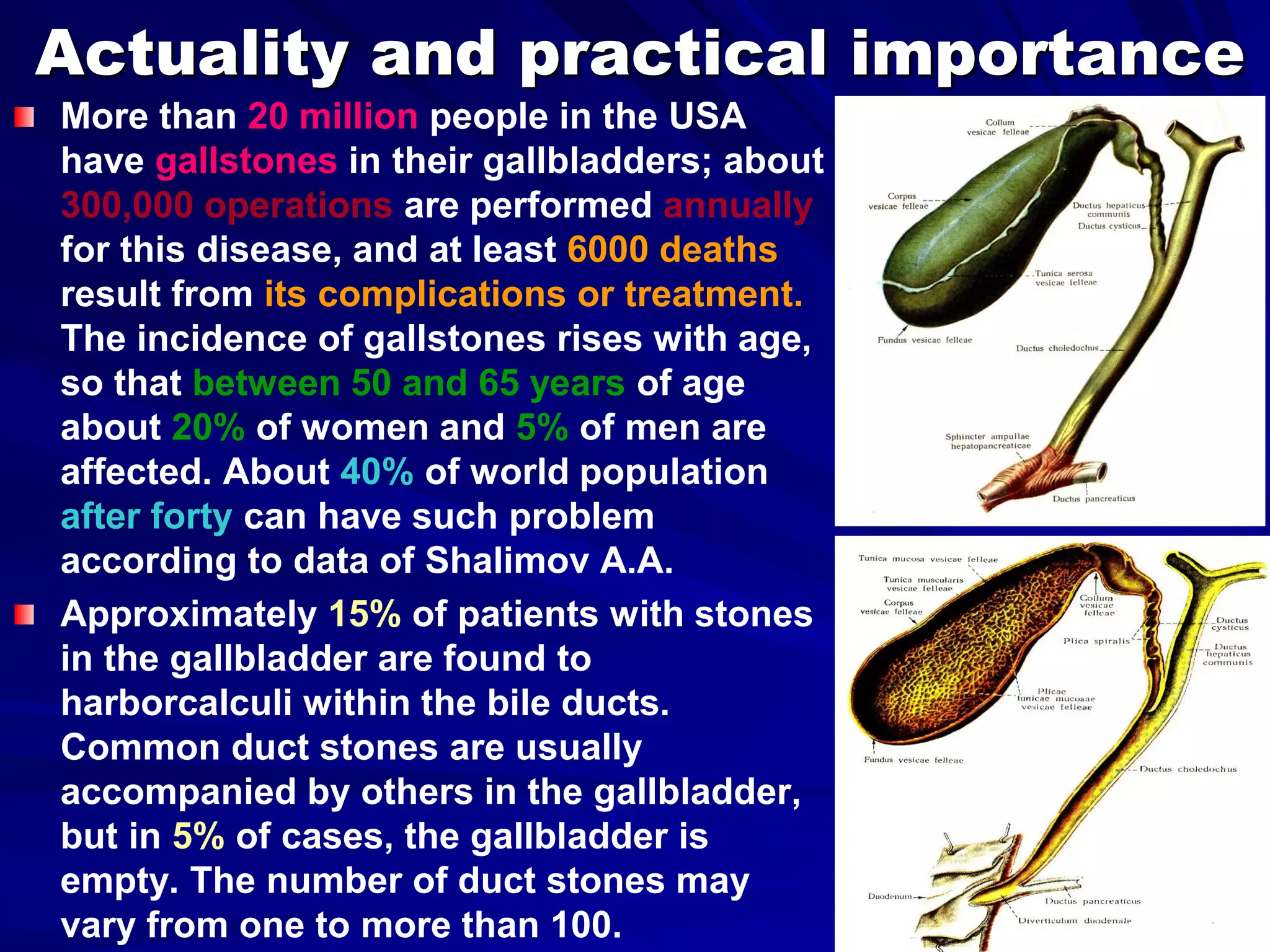
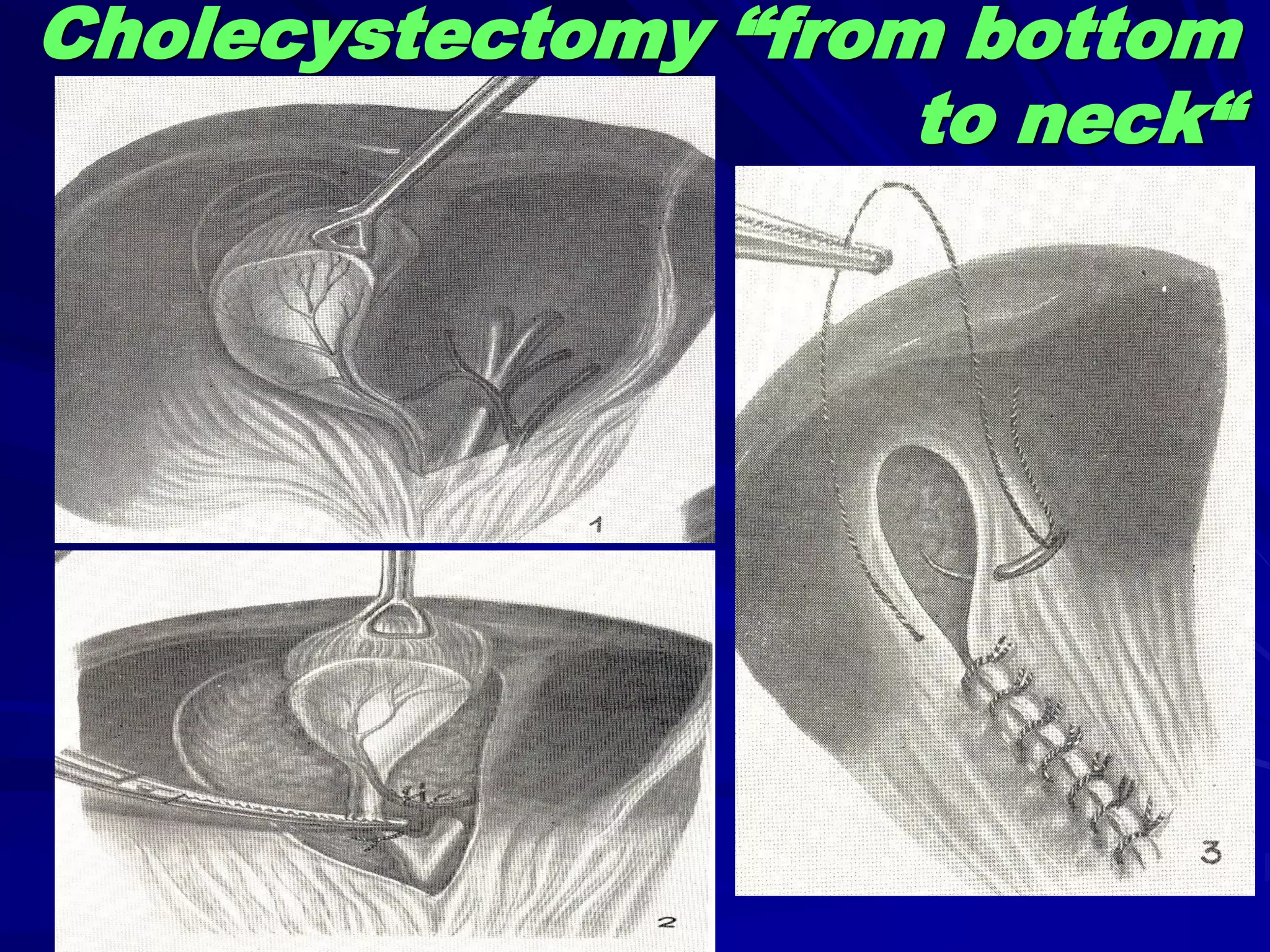
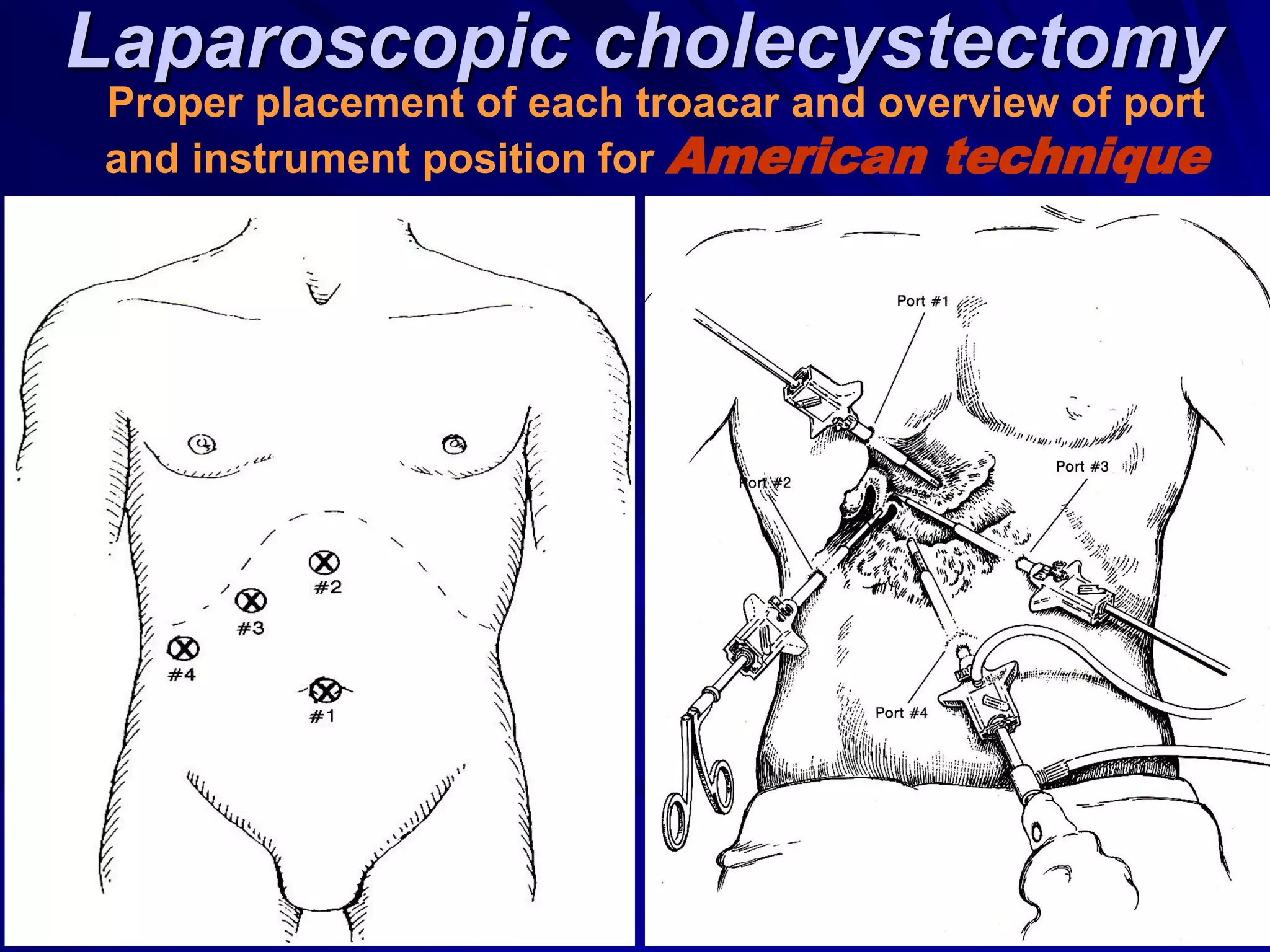

1) Gallstones affect over 20 million Americans and cause 300,000 operations and 6,000 deaths annually from complications. The risk increases with age, with 20% of women and 5% of men over 50 affected. 2) Symptoms of gallstones/cholecystitis include pain in the right upper abdomen and back, nausea, vomiting, fever, and tenderness when pressing on the right costal margin or xiphoid process. 3) Treatment options include stone dissolution, lithotripsy, laparoscopic cholecystectomy (removal of the gallbladder through small incisions), and open or laparoscopic surgery on the biliary ducts to remove stones or correct strictures.












































































