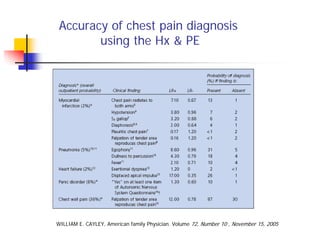
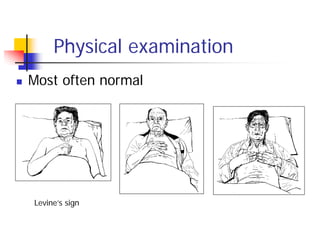
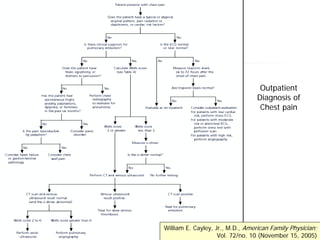
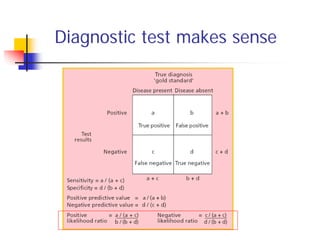
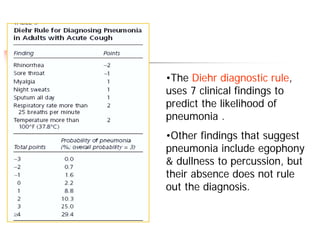
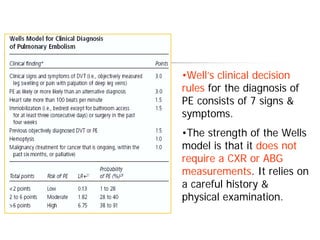
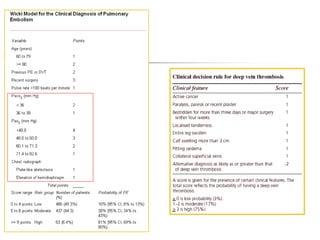
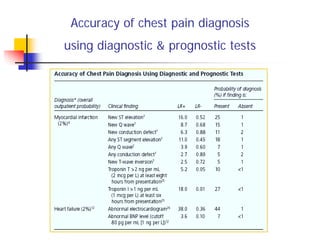
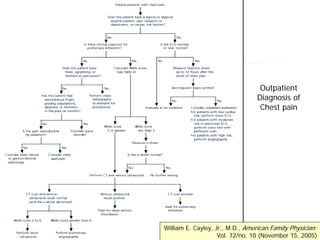
Chest pain has many potential causes, both cardiac and non-cardiac. A thorough history and physical exam are important to establish a pre-test probability of different diseases. Clinical decision rules can help quantify the likelihood of conditions like myocardial infarction, pneumonia, and pulmonary embolism. No single diagnostic test is perfect, so likelihood ratios provide a framework for interpreting test results in the context of the pre-test probability. An evidence-based approach uses all available information to guide appropriate testing and diagnosis.