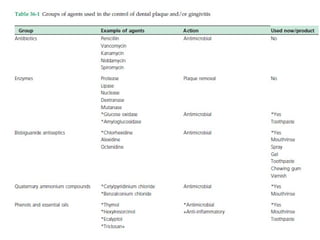
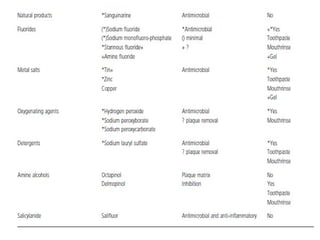
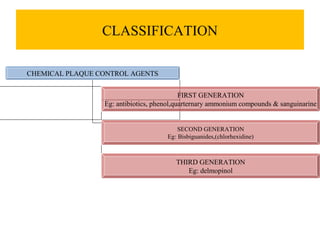
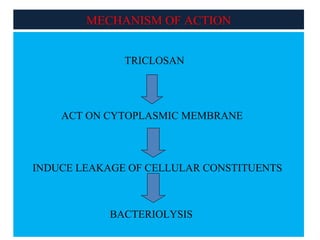
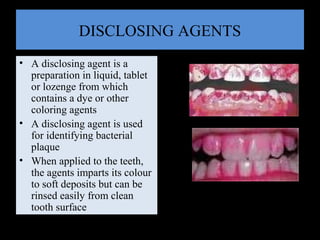
This document summarizes a seminar on chemical plaque control presented by dental students and faculty. It discusses the definitions and classifications of chemical plaque control agents. First generation agents include antibiotics, phenols, and quaternary ammonium compounds. Second generation includes bisbiguanides like chlorhexidine, and third generation includes delmopinol. The mechanisms of action and properties of various agents are described, including triclosan, metallic ions, chlorhexidine, and enzymes. Dentifrices and disclosing agents used for plaque control are also summarized.