Downloaded 120 times







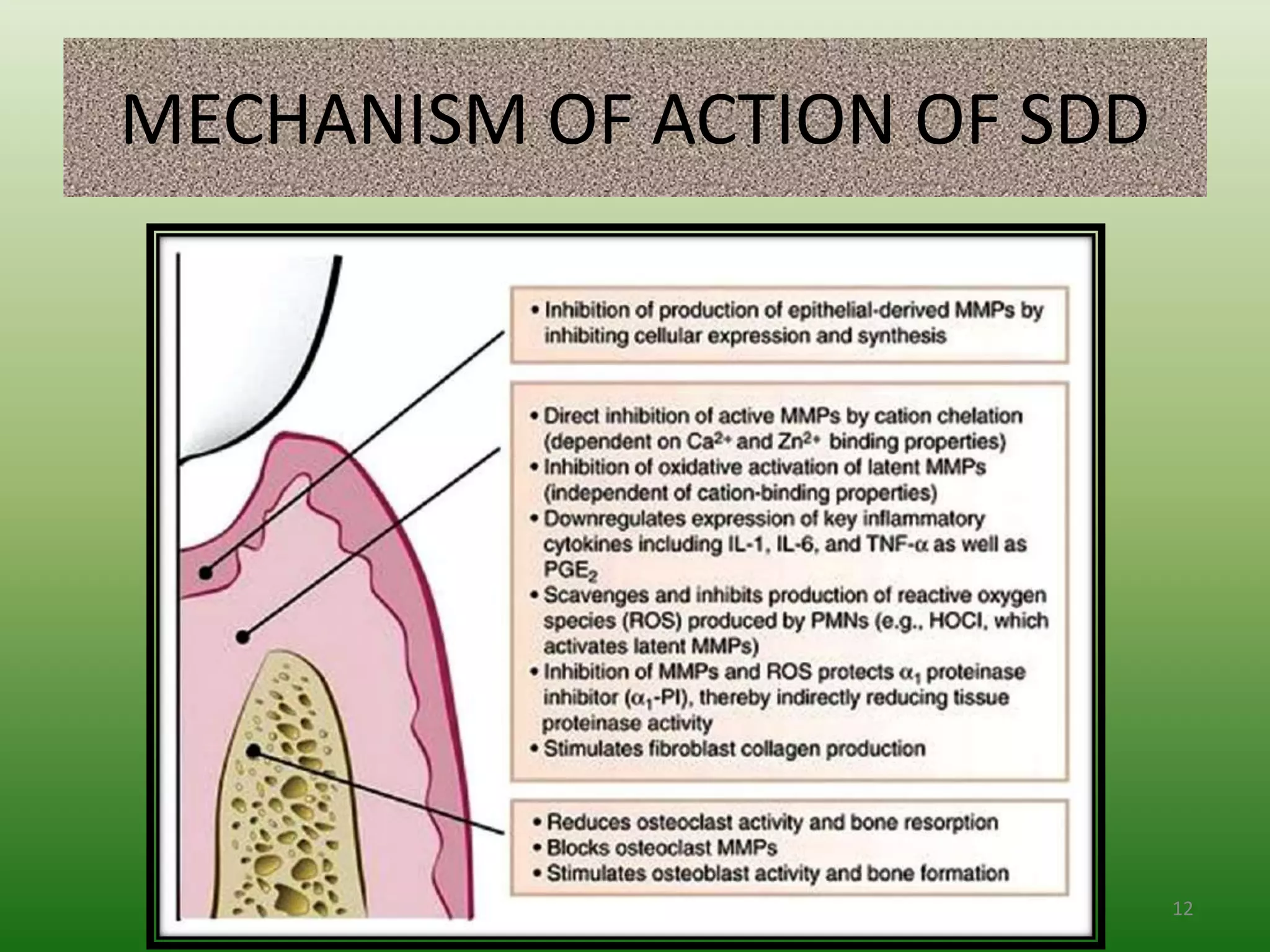







The document discusses sub-antimicrobial-dose doxycycline (SDD) as a host-modulating therapy aimed at treating chronic and aggressive periodontitis by downregulating destructive host responses and promoting tissue regeneration. SDD is administered at a dose of 20mg twice daily and is indicated as an adjunct to scaling and root planing, but not as a standalone therapy. The use of SDD can improve treatment outcomes in periodontal therapy, especially when combined with other treatment methods.