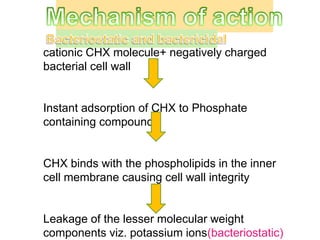
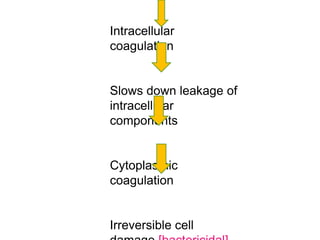
This document provides a history of oral hygiene practices and the development of mouthwashes. It focuses on chlorhexidine, detailing its discovery in the 1940s, structure, mechanism of action, properties, uses, toxicity, side effects, and alternatives. Chlorhexidine is highlighted as the gold standard for chemical plaque control due to its bacteriostatic and bactericidal properties against a broad spectrum of microorganisms. Its mechanism of action involves preventing pellicle formation and bacterial adhesion to teeth. It has high substantivity allowing effects to last over 12 hours.
















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)