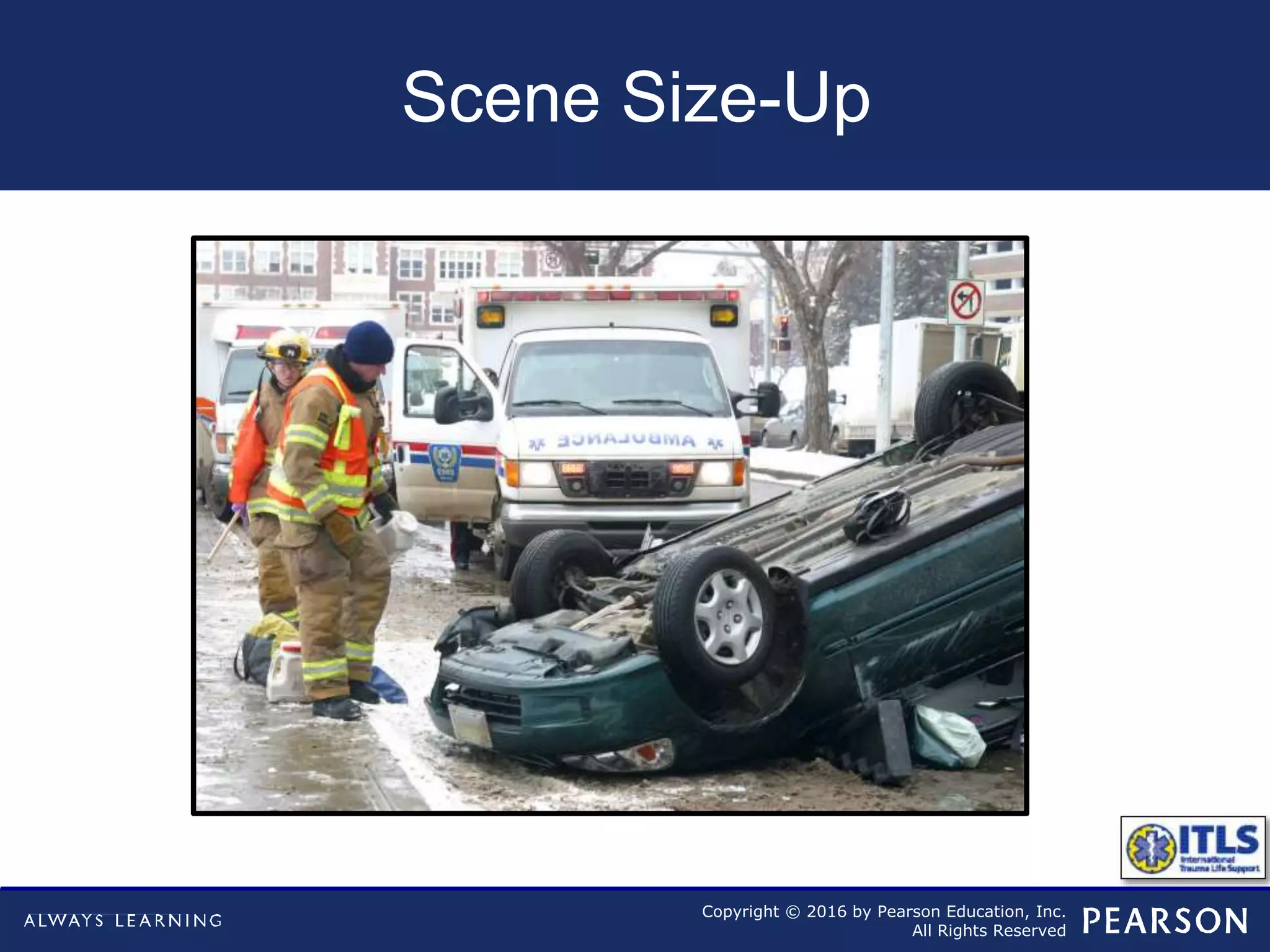
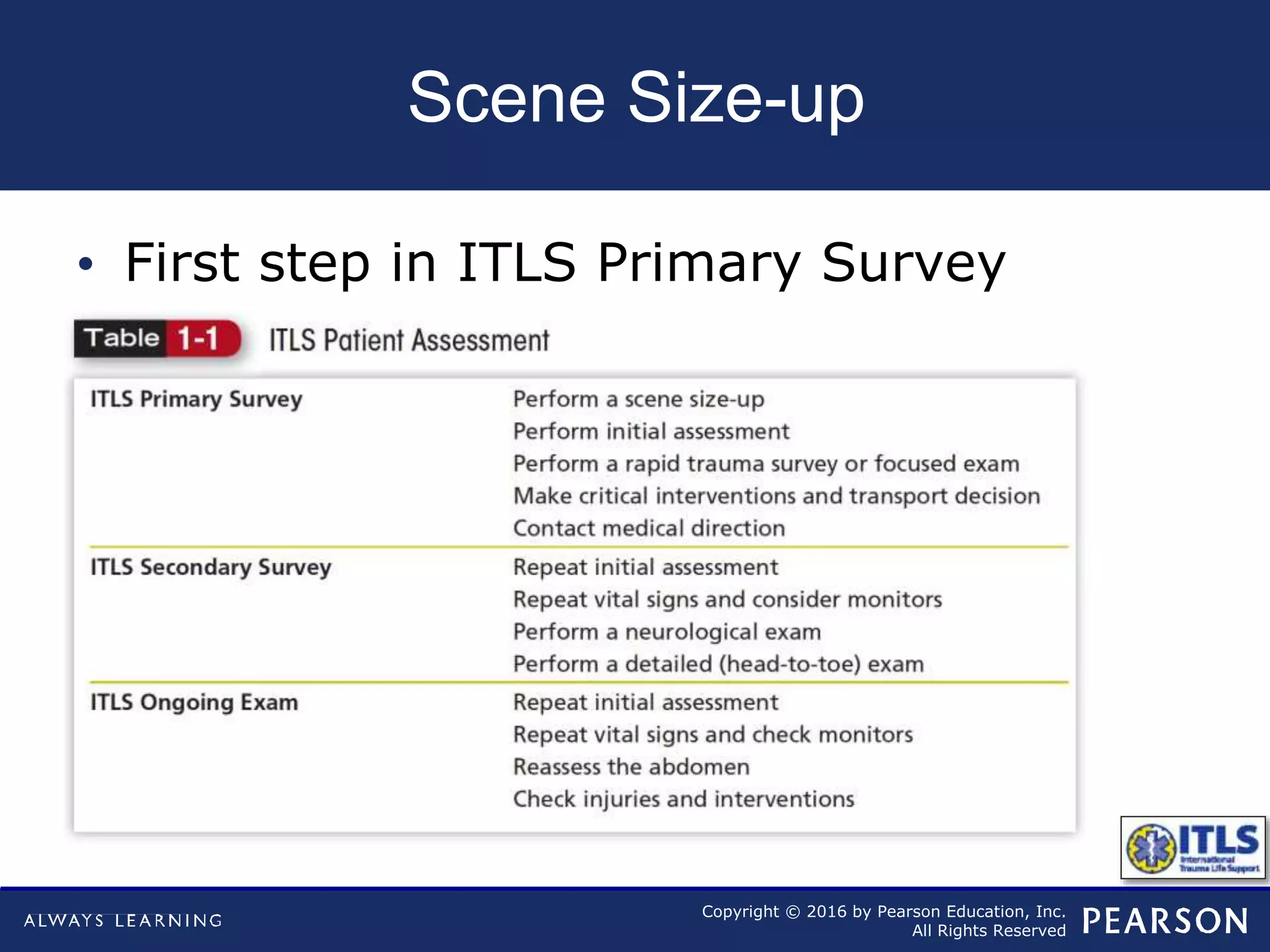
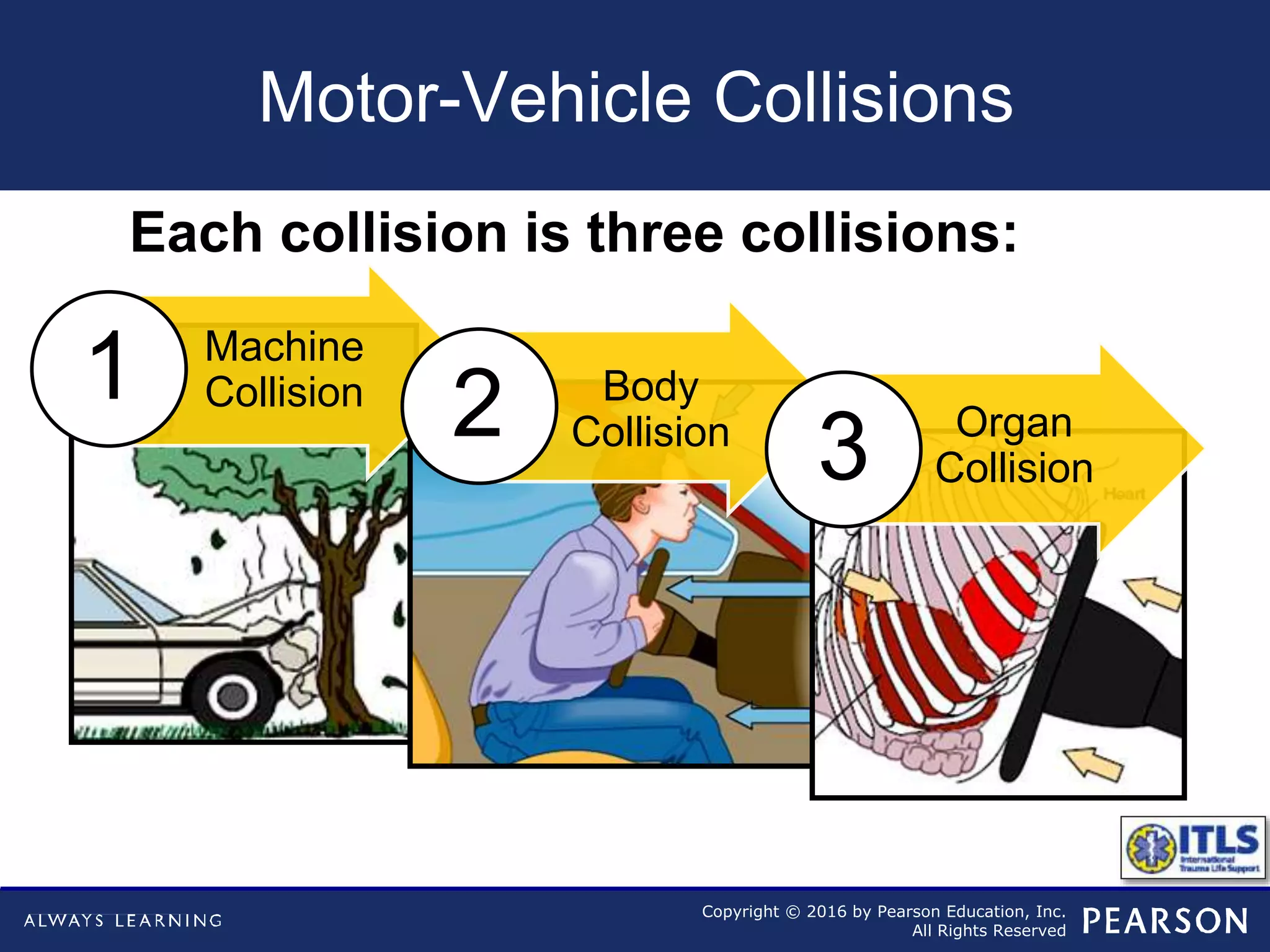
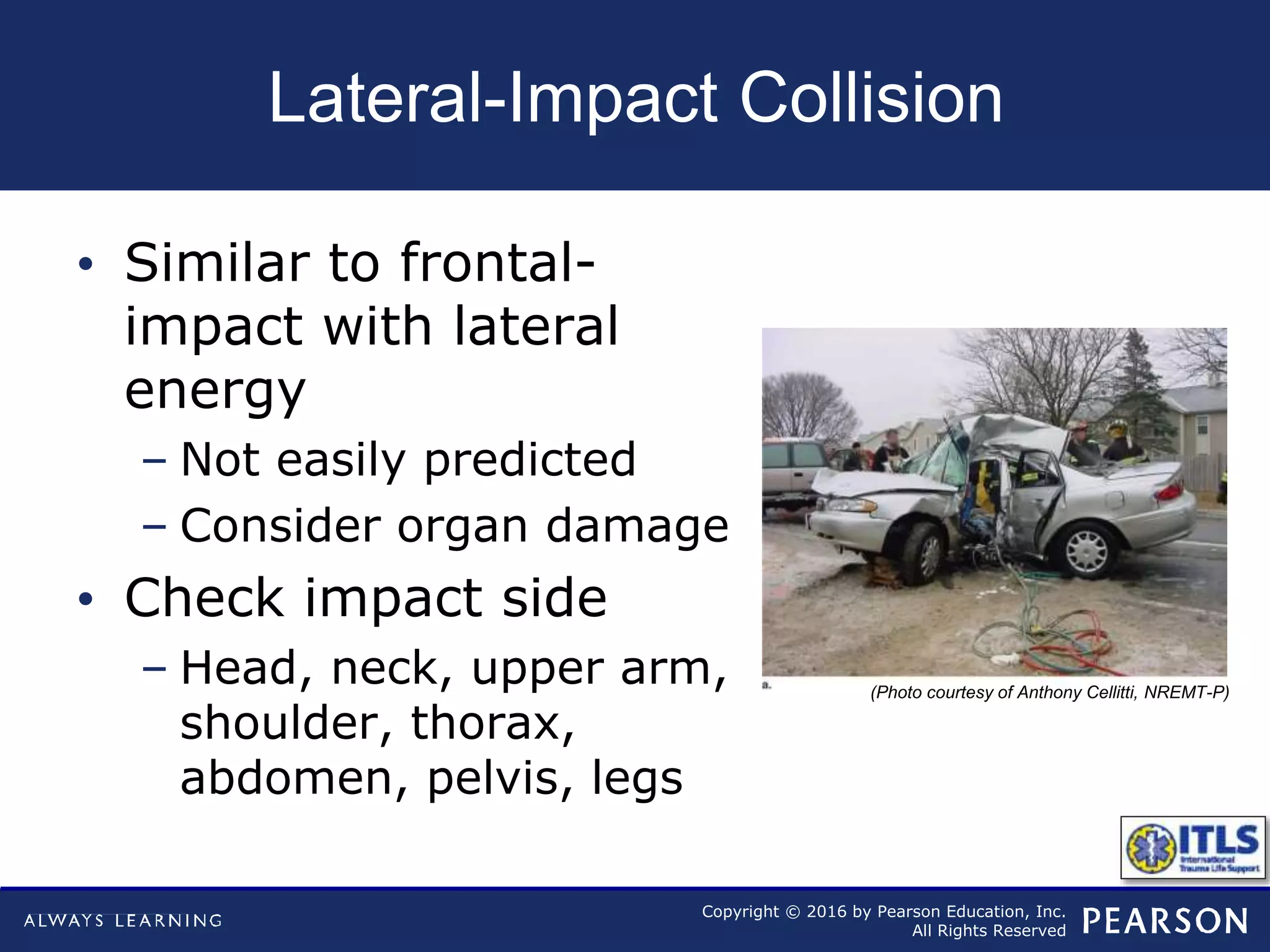
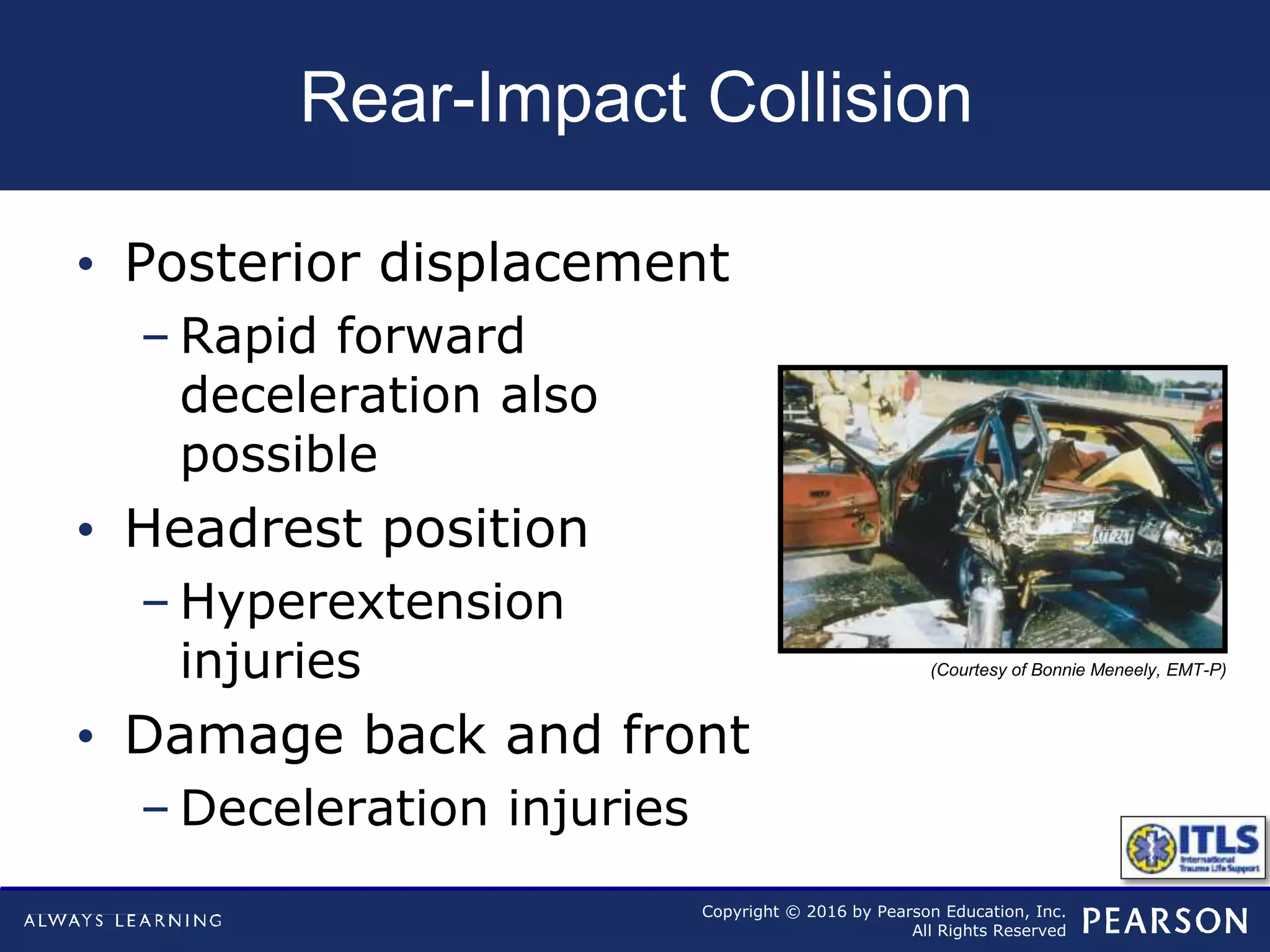
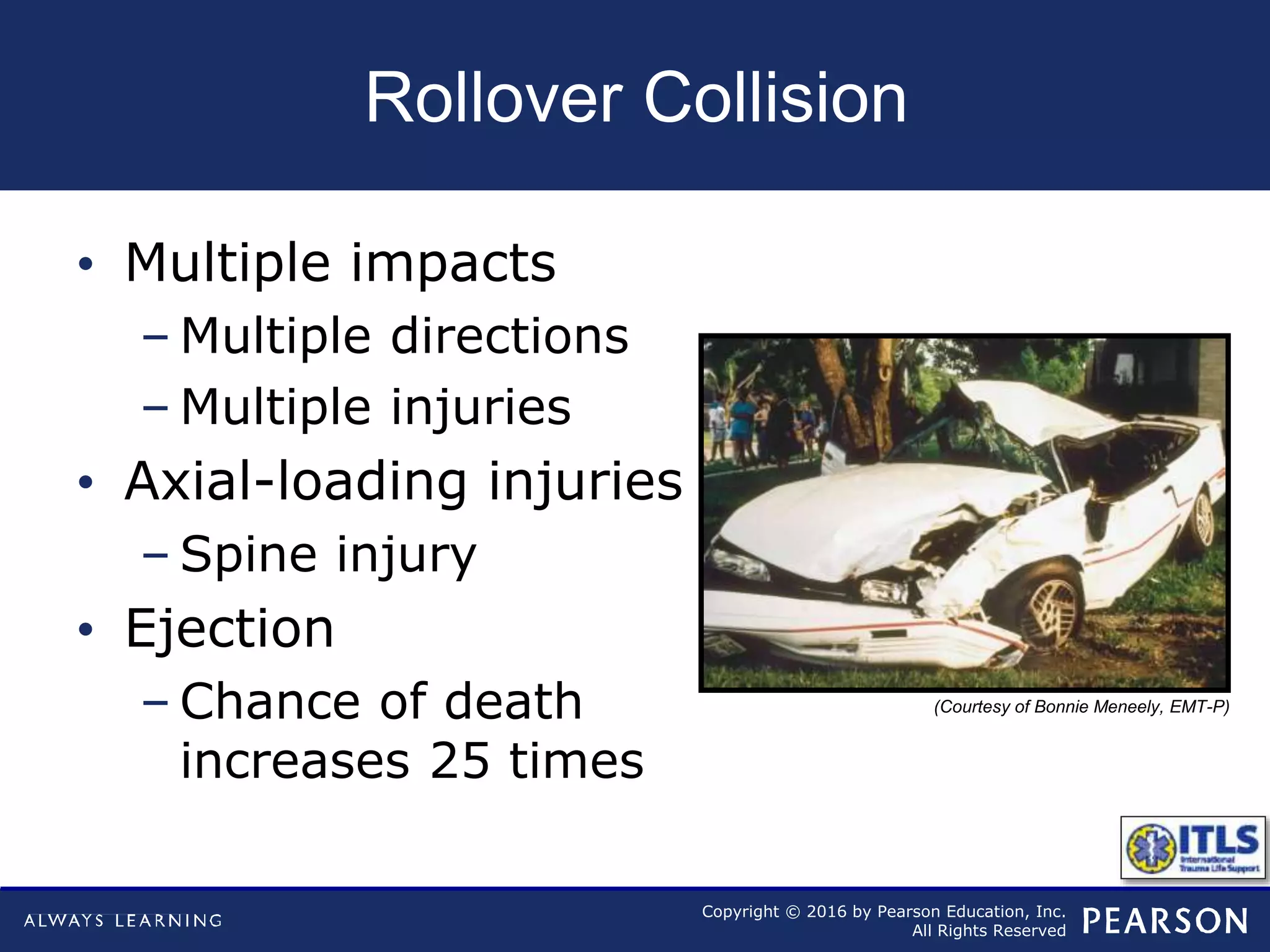
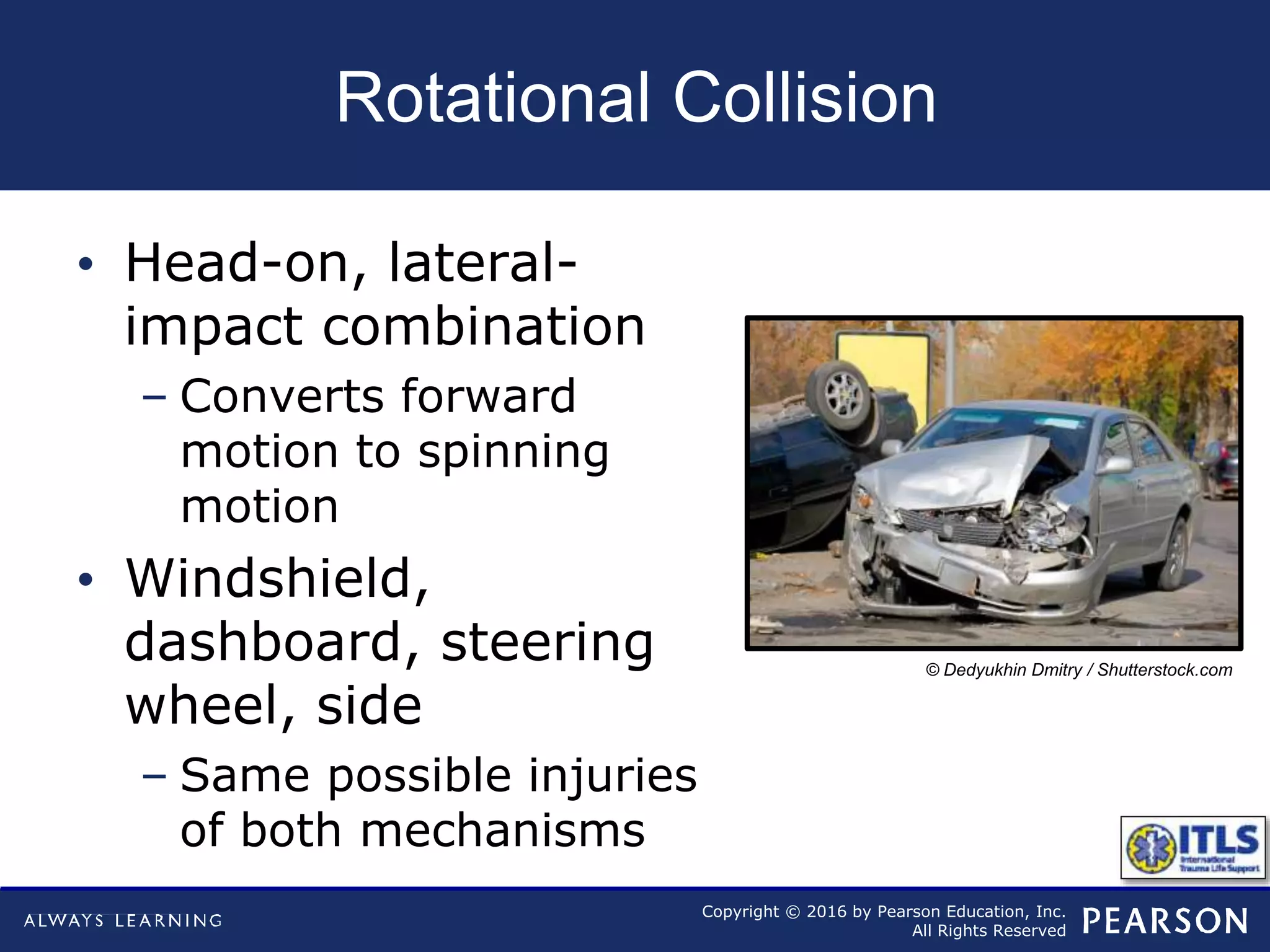
Scene size-up is the first step of trauma assessment and involves evaluating scene safety, initial triage needs, additional resource requirements, and mechanism of injury. Understanding the mechanism, such as in motor vehicle collisions, falls, or penetrating injuries, allows providers to anticipate potential injuries based on the forces involved. Proper scene size-up is critical for effective trauma management and patient care.