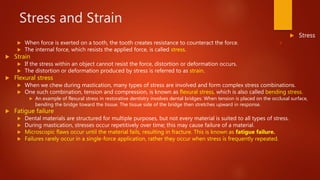
The document discusses factors of the oral environment that impact dental materials, including moisture, acid levels, temperatures, and stresses. It explains that materials used in the mouth must be biocompatible, durable, and withstand these conditions. It also discusses how forces like compression, tension, and shearing stresses affect dental structures and materials.






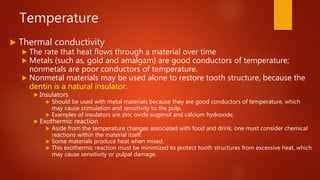
![Thermal Properties of Tooth and
Restorative Structures
Structure Coefficient of Thermal
Expansion (x 𝟏𝟎−𝟔/ºC)
Thermal Conductivity
(k [mcal cm]/𝒄𝒎 𝟐secºC)
Enamel 11 2.0
Dentin 8 1.30
Amalgam 20-28 54
Gold 15 350
*Porcelain 15 2.50
*Composite
Resin
26-40 2.60](https://image.slidesharecdn.com/oralenvironment-200716154939/85/Chapter-2-Oral-Environment-18-320.jpg)