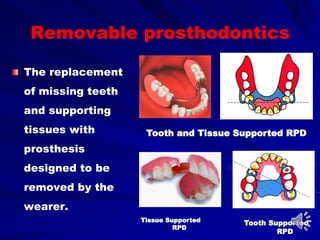
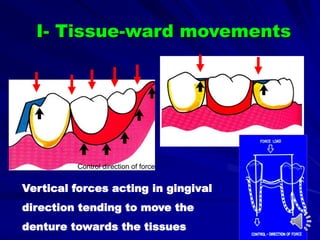
This document discusses the forces acting on removable partial dentures (RPD) and their impact on oral health. It emphasizes the objectives of RPDs, such as preserving remaining tissues, improving aesthetics, and restoring function, along with the biomechanical principles involved in their design. The document also outlines the various movement types and forces that RPDs must counteract to ensure stability and comfort for the wearer.