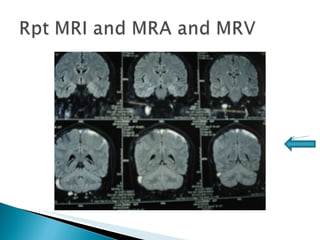
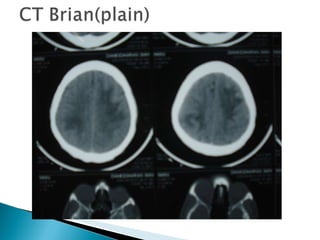
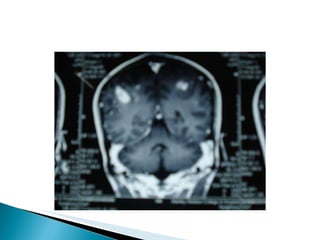
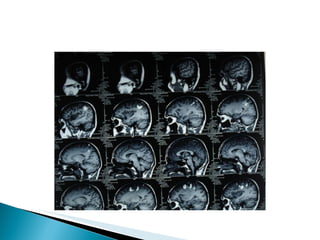
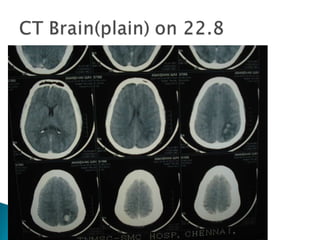
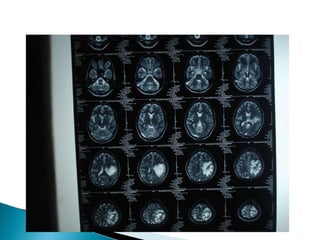
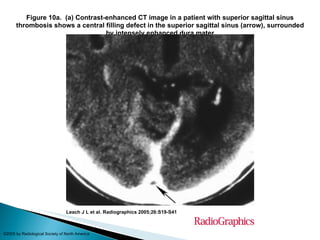
A 37-year-old male painter was admitted due to seizures and headache. CT scan showed multiple hemorrhagic infarcts in both brain hemispheres. Further imaging revealed superior sagittal sinus and bilateral transverse sinus thrombosis. The patient was started on anticoagulation therapy and made a good recovery.