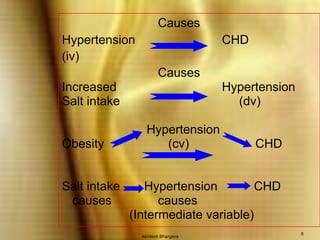
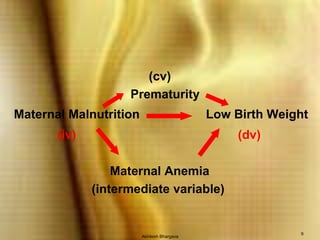
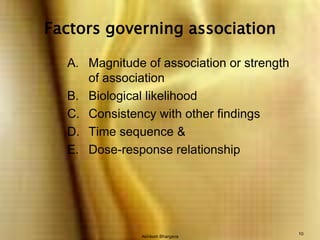
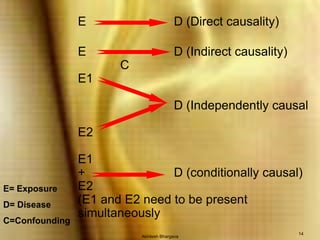
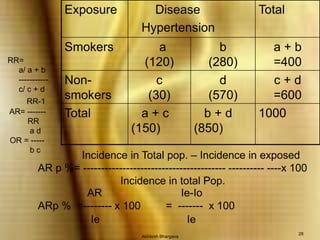
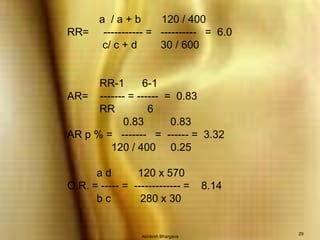

The document discusses concepts related to measuring associations between exposures and diseases in epidemiology. It defines different types of associations and measures of association, including relative risk, odds ratio, and attributable risk. It explains that an association between two variables does not necessarily imply causation and discusses several approaches used in epidemiology to help establish whether an observed association may be causal.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










