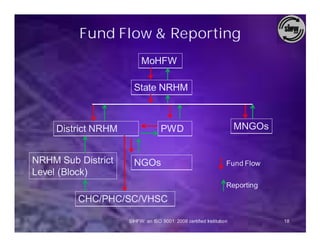
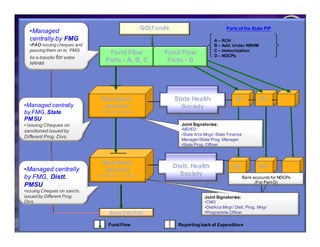
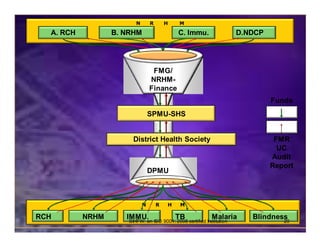
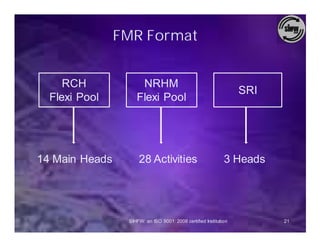
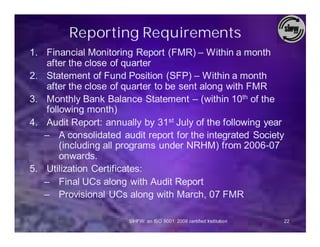
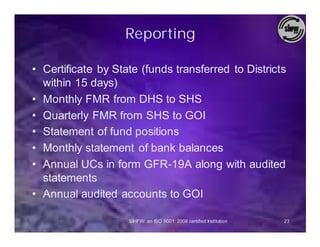
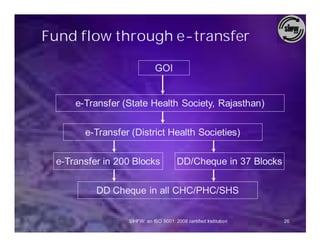
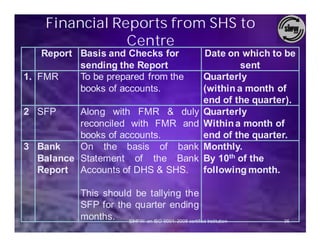
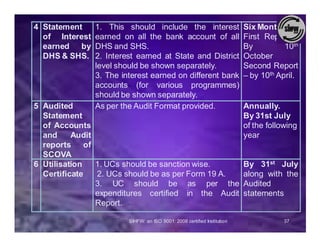

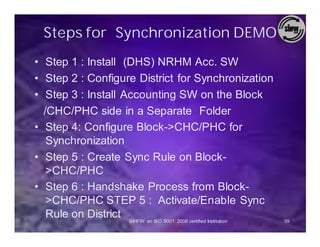
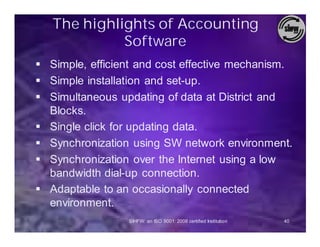



The document discusses financial management guidelines under the National Rural Health Mission (NRHM) in India. It outlines the establishment of the Financial Management Group (FMG) to coordinate accounting procedures and ensure institutions follow FMG guidelines. It describes the fund flow process from central government to states to districts and below, and the various reporting requirements back up the chain including financial monitoring reports, utilization certificates, and audit reports. It also covers accounting tools and standards, and mechanisms to monitor funds.























































































