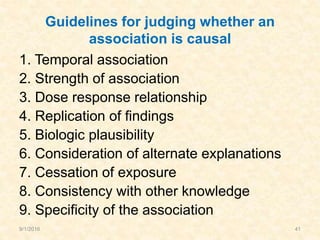
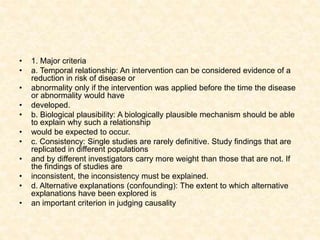
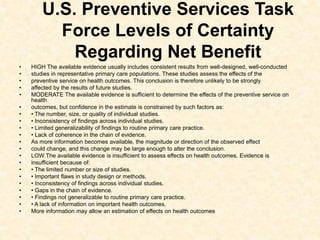
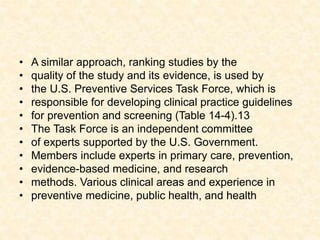
Downloaded 33 times

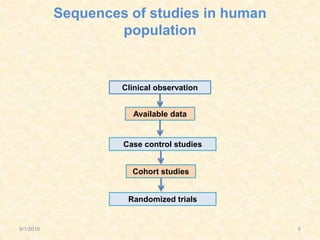
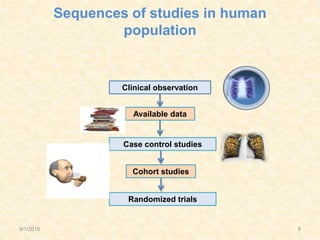



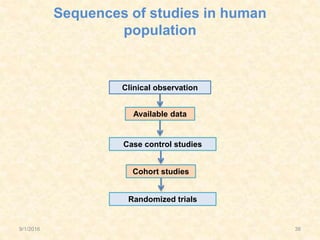
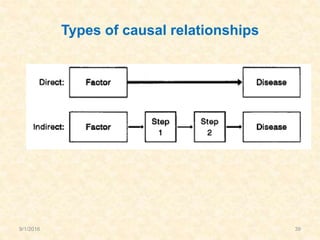
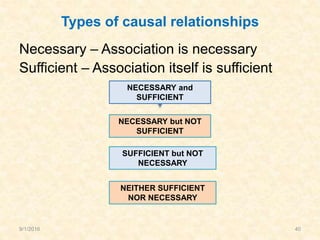



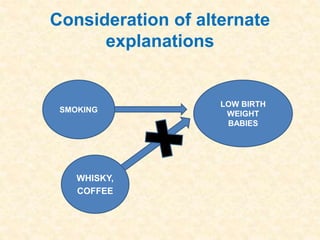
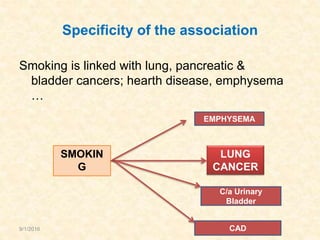
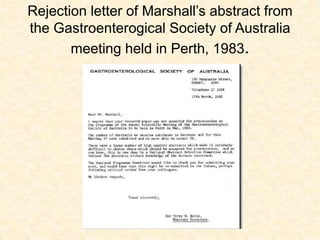

The document discusses approaches for studying disease etiology, including observational studies like ecological, cohort, and case-control studies as well as randomized trials. It also examines how evidence for a causal relationship between a factor and disease has been established through a sequence of studies, from initial clinical observations to randomized trials. Key figures in establishing causal relationships for various diseases are also mentioned, such as Alton Ochsner's work linking smoking to lung cancer and Barry Marshall and J. Robin Warren's discovery of H. pylori's role in peptic ulcers. Guidelines for determining causation, such as those from the Surgeon General and Bradford Hill, are also reviewed.










































































