Cataract
•Download as DOCX, PDF•
7 likes•3,334 views

A cataract is a cloudy area in the lens of the eye that develops slowly and causes vision to deteriorate. It occurs when proteins in the lens clump together, preventing clear images from reaching the retina. Cataracts are very common in older adults, with over half of those over 80 having them. The cloudy lens can be surgically removed and replaced with an artificial lens to restore vision.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cataract
Similar to Cataract (20)
Recently uploaded
Recently uploaded (20)
Cataract
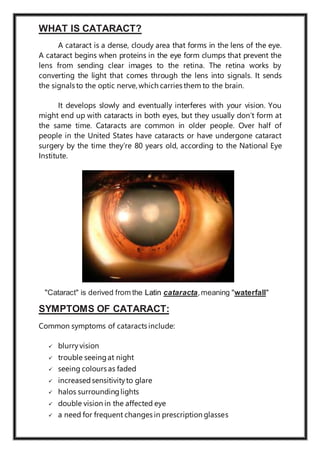
- 1. WHAT IS CATARACT? A cataract is a dense, cloudy area that forms in the lens of the eye. A cataract begins when proteins in the eye form clumps that prevent the lens from sending clear images to the retina. The retina works by converting the light that comes through the lens into signals. It sends the signals to the optic nerve, which carries them to the brain. It develops slowly and eventually interferes with your vision. You might end up with cataracts in both eyes, but they usually don’t form at the same time. Cataracts are common in older people. Over half of people in the United States have cataracts or have undergone cataract surgery by the time they’re 80 years old, according to the National Eye Institute. "Cataract" is derived from the Latin cataracta,meaning "waterfall" SYMPTOMS OF CATARACT: Common symptoms of cataracts include: blurryvision trouble seeingat night seeing colours as faded increasedsensitivityto glare halos surroundinglights double vision in the affected eye a need for frequent changes in prescription glasses
- 2. CAUSES OF CATARACTS: Age: lens proteins denature and degrade over time, and this process is accelerated by diseases such as diabetes mellitus and hypertension. There is loss of protective and restorative mechanism due to alteration in gene expression and chemical processes within the eye. Trauma: blunt trauma causes swelling, thickening, and whitening of the lens fibers. While the swelling normally resolves with time, the white colour may remain. Radiation: Ultraviolet light has been shown to cause cataracts, and some evidence indicates sunglasses worn at an early age can slow its development in later life. Microwave radiation has also been found to cause cataracts. Genetics: genetic component is strong in the development of cataracts, most commonly through mechanisms that protect and maintain the lens. The presence of cataracts in childhood or early life can occasionallybe due to a particular syndrome. Smoking and alcohol: Cigarette smoking has been shown to double the rate of nuclear sclerotic cataracts and triple the rate of posterior sub capsular cataracts. Inadequate vitamin C: low vitamin C intake and serum levels have been associatedwith greater cataractrates. Medications: some medications, such as systemic, topical, or inhaled corticosteroids may increase the risk of cataract development. Post-operative: nearly every person who undergoes a vitrectomy—without ever having had cataract surgery—will experience progression of nuclear sclerosis after the operation.
- 3. PATHOPHYSIOLOGY OF CATARACT: The clear lens of the eye transmits light rays entering the eye and focuses them on retina With ageing lens proteins progressively denature causing increase in density and yellowish-brown coloration of the lens. Other factors such as blunt force trauma can cause thickeningand irreversible whiteningof the lens. The resultant cloudy lens lacks the ability to transmit and focus light rays on the retina. This manifests as blurry vision or loss of vision in advancedcases.
- 4. TYPES OF CATARACTS: Nuclear cataracts form in the middle of the lens and cause the nucleus,or the centre, to become yellow or brown. Cortical cataracts are wedge-shaped and form around the edges of the nucleus. Posterior capsular cataracts form faster than the other two types and affect the back of the lens. Congenital cataracts, which are present at birth or form during a baby’s first year, are less common than age-relatedcataracts.
- 5. Secondary cataracts are caused by disease or medications. Diseases that are linked with the development of cataracts include glaucoma and diabetes. The use of the steroid prednisone and other medications can sometimes lead to cataracts. Traumatic cataracts develop after an injury to the eye, but it can take several years for this to happen. Radiation cataracts can form after a person undergoes radiation treatment for cancer.
- 6. RISK FACTORS OF CATARACT: older age heavy alcohol use smoking obesity high blood pressure previous eye injuries a familyhistory of cataracts too much sun exposure diabetes exposure to radiation fromX-rays and cancer treatments DIAGNOSTIC STUDIES: Your doctor will perform a comprehensive eye exam to check for cataracts and to assess your vision. It includes:- Visual acuity test – this eye chart test measures how well you see at various distances. Pupil dilatation – the pupil is widened with eye drops to allow your eye doctor to see more of the lens and retina and look for other eye problem. Tonometry – standard test to measure fluid pressure inside the eye. The most common tonometry test uses a painless puff of air to flatten your cornea and test your eye pressure. Your doctor will also put drops in your eyes to make your pupils bigger. This makes it easier to check the optic nerve and retina at the back of your eye for damage. Other tests your doctor might perform include checking your sensitivity to glare and your perception of colours.
- 7. TREATMENT FOR CATARACT: If you’re unable or uninterested in surgery, your doctor may be able to help you manage your symptoms. They may suggest stronger eyeglasses,magnifying lenses, or sunglasses with an anti-glare coating. Surgery: recommended when cataracts prevent you from going about your daily activities, such as reading or driving. It’s also performed when cataracts interfere with the treatment of other eye problems. Phacoemulsification, most common method of removal. Phaco involves a small incision on the side of the cornea. A tiny probe is inserted which emits ultrasound waves that softens and break up the cloudy centre of the lens so it can be removed with suction. Extracapsular surgery involves removing the cloudy part of the lens through a long incision in the cornea. After surgery, an artificial intraocular lens is placed where the natural lens was. Surgery to remove a cataract is generally very safe and has a high success rate. Most people can go home the same day as their surgery.
- 8. Postoperative care The postoperative recovery period (after removing the cataract) is usually short. The patient is usually ambulatory on the day of surgery, but is advised to move cautiously and avoid straining or heavy lifting for about a month. The eye is usually patched on the day of surgery and use of an eye shieldat night is often suggested for several days after surgery. In all types of surgery, the cataractous lens is removed and replaced with an artificial lens, known as an intraocular lens, which stays in the eye permanently. Intraocular lenses are usually monofocal, correcting for either distance or near vision. Multifocal lenses may be implanted to improve near and distance vision simultaneously, but these lenses may increase the chance of unsatisfactoryvision.
- 9. COMPLICATIONS OF CATARACT: Rupture of the posterior capsule during surgery, which may result in the nucleus dropping back into the vitreous cavity, necessitating a further procedure (vitrectomy) either during the surgery or later. Posterior capsule rupture may also result in the need to use a differenttype of intraocular lens in the eye; Raised intraocular pressure owing to the blockage of aqueous humour outflow channels with the viscoelastic substance used at surgery. Pressure may also rise as a reaction to the surgery or as a result of inflammation. The patient is likely to experience pain and new blurringof vision some hours after surgery; A shallow anterior chamber, which may result from inhibition of aqueous humour production because of a wound leak following postoperative trauma, or from raised pressure. This is of concern, because if the chamber becomes very shallow, the corneal endothelium may touch the iris. Damage to corneal endothelial cells may result in permanentcorneal oedema; Retinal detachment may occur after cataract surgery in a very small number of cases. Any report by the patient of new floaters in the eye, flashing lights or the loss of sectors of vision indicates that an urgent examination is required; Cystoids macular oedema (oedema of the retina at the macular) is likely to cause some disturbance of central vision. It often disappears over time; Uveitis (inflammation of the iris and ciliary body) occurs as an inflammatory response to surgery. It is a normal consequence of surgery and patients are treated postoperatively with eye drops containing a steroid to reduce and control the inflammation. Pain and redness of the eye may occur if the inflammation increases, in which case modification of the drop therapyis required; Displacement of the intraocular lens may occur after surgery and is likely to necessitate further surgical intervention to replace the lens or correctits position; Posterior capsular opacification is the most frequent long-term complication of surgery The posterior portion of the remaining lens capsule becomes opacified and the patient reports reduction in vision. Posterior capsular opacities are easily dealt with using a laser to burn a hole in the capsule (YAG capsulotomy). This is painless, and can easilybe undertaken as an outpatient procedure;
- 10. Infection is always a possible complication of surgery, and for this reason a prophylactic antibiotic drop will be prescribed after cataract extraction. The anti-inflammatory and the antibiotic may be combinedin a single drop such as Maxitrol. PREVENTION FOR CATARACT: protect your eyes from UVB rays by wearingsunglasses outside have regular eye exams stop smoking eat fruits and vegetables that contain antioxidants maintain a healthy weight keep diabetes and other medical conditions in check
- 11. NURSING ASSESSMENT: Test papillary response. Examine cornea to rule out any opacities. Examine ocular adnexa. Performdilated fundus examination. PerformUSG B-scan. Measure intraocular pressure. Performpotential acuitymeasurement. Performbiometry. NURSING DIAGNOSIS: Anxiety related to lack of knowledge – Interventions - Assess the degree and duration of visual impairment. Encourage conversation to find out the patient's concerns, feelings, and the level of understanding. Orient the patient to the new environment. Explain the preoperative routines. Encourage participation of family or the people who matter in patient care. Push to perform dailyliving habits when able. Risk for injuryrelated to blurredvision – Interventions - Help the patient when able to do until postoperative ambulation and achieve stable vision and adequate coping skills, using techniques of vision guidance. Help the patient set the environment. Orient the patient in the room. Do not put pressure on the affectedeye trauma. Use proper procedures when providingeye drugs. Acute pain related to trauma to the incision andincreasedIOP – Interventions - Assess the degree and duration of pain. Encourage use of sunglasses in strong light. Give cold compress on demand for blunt trauma. Give medications to control pain and the IOP as prescribed.
- 12. ROLE OF NURSE IN CATARACT: Although the care of patients with a cataract is a multidisciplinary effort, nurses are increasingly undertaking much of the care surrounding the surgical procedure. Assessment is commonly carried out in preadmission clinics, with ophthalmic nurses playing a lead role in the pre assessment of the patient, including examining the eye, performing biometry, and obtaining informed consent. Ophthalmic nurses also undertake a key role in theatre, including the giving of sub-Tenon’s anaesthesia and acting as first assistant to the ophthalmologist - a longstanding role within this specialty. Nurses undertake all postoperative care of patients who have had uncomplicated cataract surgery and this may include the modification of medication using patient group directives or supplementary prescribing, auto refraction and final discharge of the patient from the service. Tell the patient to avoid activities that increase intraocular pressure such as straining. Urge the patient to protect the eye from accidental injury at night by wearing a plastic or metal shield with perforations, a shield or glasses should be worn for protection duringthe day. Advise the patient to watch for and immediately report complication such as sharp pain in the eye that’s uncontrolled by analgesics this can be caused hyphema (a clouding in the anterior chamber) and may herald an infection.
- 13. RESEARCH: N-Acetylcarnosine drops have been investigated as a medical treatment for cataracts. The drops are believed to work by reducing oxidation and glycation damage in the lens, particularly reducing crystallin cross linking. Some benefit has been shown in small manufacturer sponsored randomized controlled trials but further independentcorroboration is still required. Femtosecond laser mode-locking, used during cataract surgery, was originally used to cut accurate and predictable flaps in LASIK surgery, and has been introduced to cataract surgery. The incision at the junction of the sclera and cornea and the hole in capsule during capsulorhexis, traditionally made with a handheld blade, needle, and forceps, are dependent on skill and experience of the surgeon. Sophisticated three- dimensional images of the eyes can be used to guide lasers to make these incisions. Nd:YAG laser can also then break up the cataract as in phacoemulsification. Stem cells have been used in a clinical trial for lens regeneration in twelve children under the age of two with cataracts present at birth. The children were followed for six months, so it is unknown what the long- term results will be, and it is unknown if this procedure would work in adults.
- 14. CONCLUSION: Cataracts can interfere with daily activities and lead to blindness when left untreated. Although some stop growing, they don’t get smaller on their own. The surgical removal of cataracts is a very common procedure and is highly effective roughly 90% of the time, according to the National Eye Institute. BIBLIOGRAPHY: